


Figure 02: Red arrow shows the division of the sciative nerve and the blue arrow shows the femoral vascular-nervous bundle.

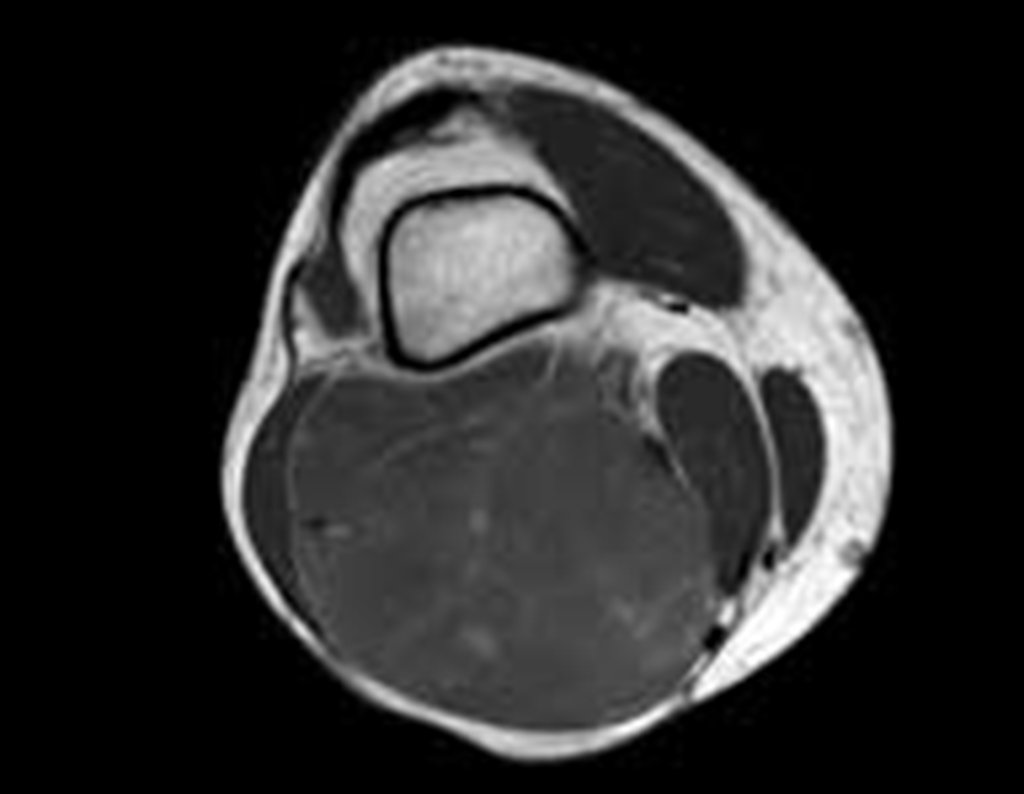
Figure 04: Extension of the injury to the posterior region of the knee.



Figure 7: Septate lesion in close contact with the vascular-nervous bundle.

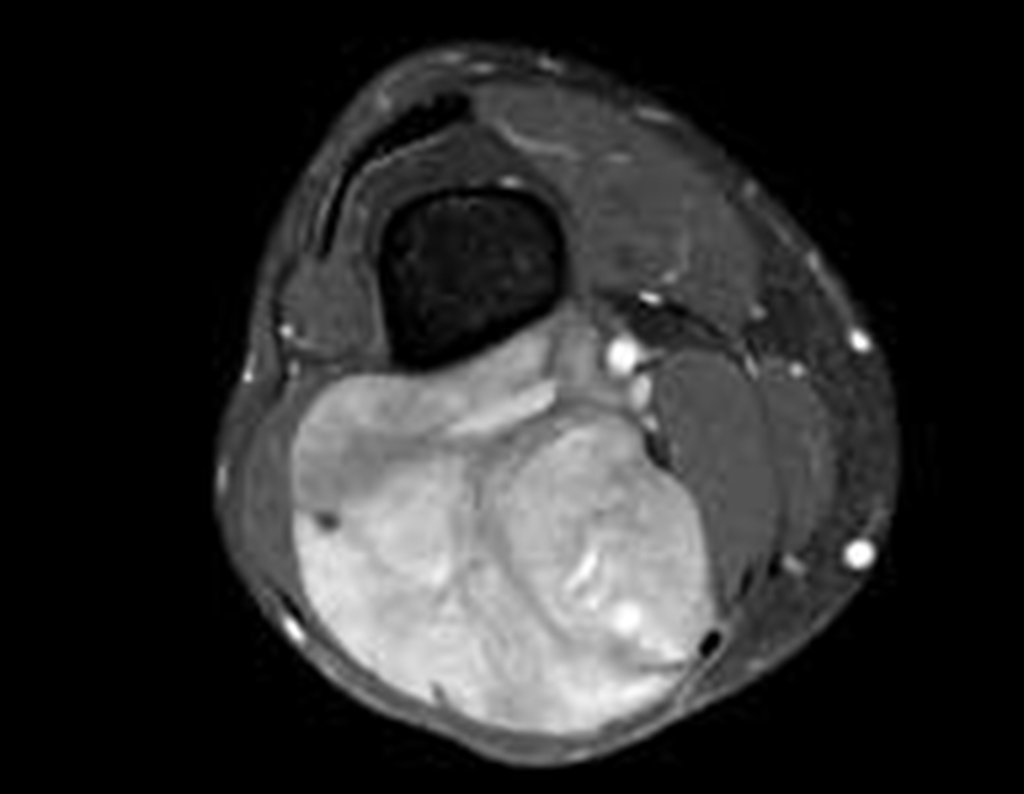
Figure 9: Great heterogeneity of the lesion.





























