











It includes academic lectures, presentations from national and international congresses, published papers, case discussions, performed surgical procedures, and proprietary techniques developed.
The digital format was chosen because the web allows the inclusion of texts with numerous visual resources, such as images and videos, which would not be possible in a printed book.
The content is intended for students, healthcare professionals, and the general public interested in the field.
The search for biological solutions that make it possible to resolve bone defects, caused by locally aggressive tumor or pseudotumor lesions, congenital malformations, traumas and infections, has increasingly aroused the interest of orthopedists(1).
Advances in therapeutic resources in the treatment of malignant bone tumors have provided greater survival and even the prospect of a cure for patients. On the other hand, there is the inherent complication of endoprostheses over time. The correlation of these factors therefore requires the improvement of biological reconstruction methods that aim to be definitive(1-4). Reviewing the literature regarding bone reconstructions in the developing skeleton, it can be seen that this subject is of current interest(1,2,4-6).
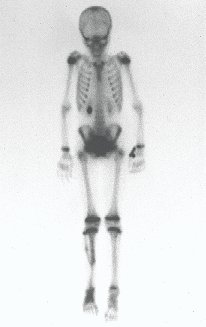
In February 1999, the nine-year-old male LCAA patient was undergoing preoperative chemotherapy treatment for diaphyseal Ewing sarcoma of the right femur at the Pediatric Hematology and Oncology Service of the Department of Pediatrics and Child Care of Santa Catarina. Casa Misericórida de São Paulo.
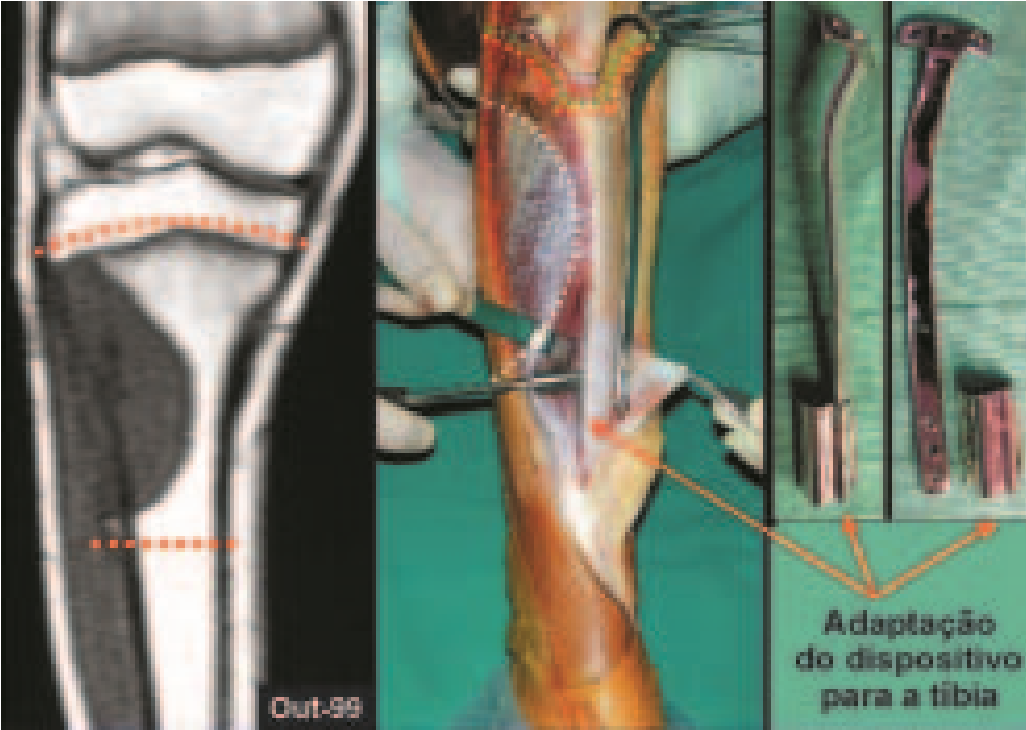
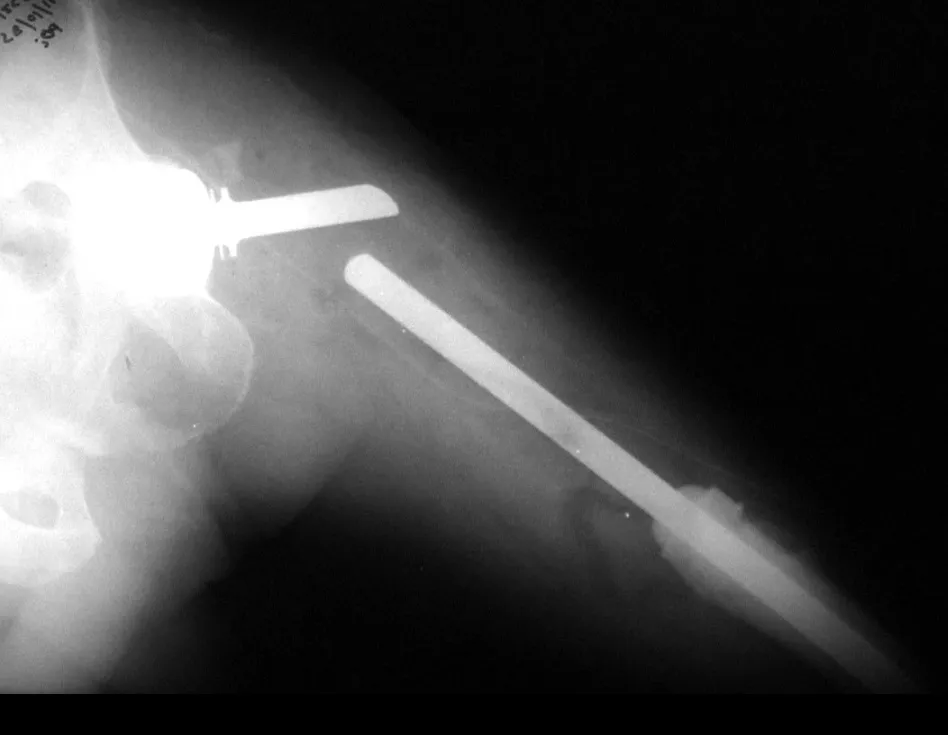
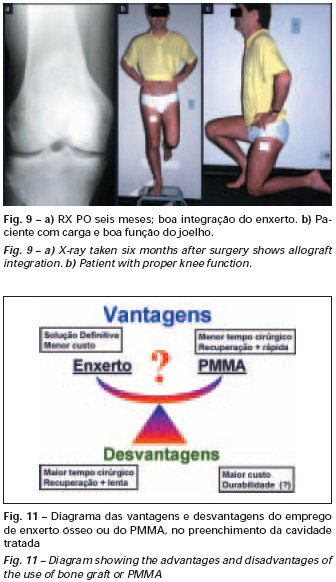
We currently use this device for immediately extensible internal fixation, and it currently consists of a single piece that has a curved side flap to adapt to the femur and humerus or it can be flat with an angle to adapt to the shape. triangular shape of the tibia (fig. 9). Another patient, WRC, 14 years old, with osteosarcoma of the right tibia, is a relatively recent example of reconstruction of the proximal metaphyseal segment of the tibia, with resection that also included the growth plate; We performed reconstruction with the fibula, including its epiphysis and using the epiphyseal plate of this fibula to provide growth (fig. 9). We can observe a slip of 0.75 cm by comparing the distances between the physeal plate of the transported fibula and the limit of the extensible device. Radiographic correction of the valgus inclination of the tibial plateau and clinical realignment of the knee can be seen (fig. 10). The patient is currently in the final phase of growth and has good knee function (Figs. 11 and 12).
We believe that this device for extensible internal fixation, which we developed, can be used both for the treatment of selected cases of aggressive tumor lesions and also for other conditions, such as congenital malformations and sequelae of trauma or infections, which may require reconstructions that require a stabilization mechanism that allows the epiphysis to be fixed, but without blocking bone growth.
1. Manfrini M., Gasbarrini A., Malaguti C., et al: Intraepiphyseal resection of the proximal tibia and its impact on lower limb growth. Clin Orthop 358: 111-119, 1999. 2. Eckardt JJ, Kabo JM, Kelley CM, et al: Expandable endoprosthesis reconstruction in skeletally immature patients with tumors. Clin Orthop 373: 51-61, 2000. 3. Capanna R., Bufalini C., Campanacci M.: A new technique for reconstructions of large metadiaphyseal bone defects. Orthop Traumatol 2:159-177, 1993. 4. Cool WP, Carter SR, Grimer RJ, Tillman RM, Walker PS: Growth after extendible endoprosthetic replacement of the distal femur. J Bone Joint Surg [Br] 79: 938-942, 1997. 5. Baptista PPR, Guedes A., Reggiani R., Lavieri RF, Lopes JAS: Tibialization of the distal fibula with preservation of the epiphyseal plate: preliminary report. Rev Bras Ortop 33: 841-846, 1998. 6. Baptista PPR, Guedes A., Reggiani R., Lavieri RF, Pires CEF: Tibialization of the fibula: description of the surgical approach. Rev Bras Ortop 33: 861-866, 1998.
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com
Reconstruction was performed by arthrodesing the ipsilateral distal fibular epiphysis with the talus, preserving the fibular epiphyseal plate. Preliminary postoperative evaluation using axial slice scintigraphy demonstrated signs of capture of the fibula throughout the transposed extension and at the level of the projection of the distal fibular growth plate. It is not yet possible to distinguish the hypercapture of the physeal plate from the reparative process of arthrodesis at the level of the talus. Radiographic controls from September/98, nine months after surgery, show complete integration of the transposed fibula, both proximally and distally. Thickening of the fibula is already evident and the fibular growth plate can be easily distinguished.
Osteosarcoma is the most common primary malignant bone tumor between the first and second decades of life(21). It generally affects the metaphyses of long bones, with the most common locations being the distal third of the femur and the proximal third of the tibia. Location in the distal third of the tibia represents approximately 3% of cases.
With the evolution of chemotherapy treatment, there was new encouragement in the approach to this condition, as it provided an increase in the average survival rate(2,7,19,21,22). This fact led to better improvements in the surgical techniques used until then. Malignant neoplasms previously treated with radical surgery, currently, when they respond favorably to neo-adjuvant chemotherapy, are approached with the aim of preserving the involved limb, with or without a biological solution(1,2,4,8,13,14,22). This concept has expanded, raising the expectations of the surgeon who seeks to combine the preservation of the affected body segment with the maintenance of maximum function(4,8,13).




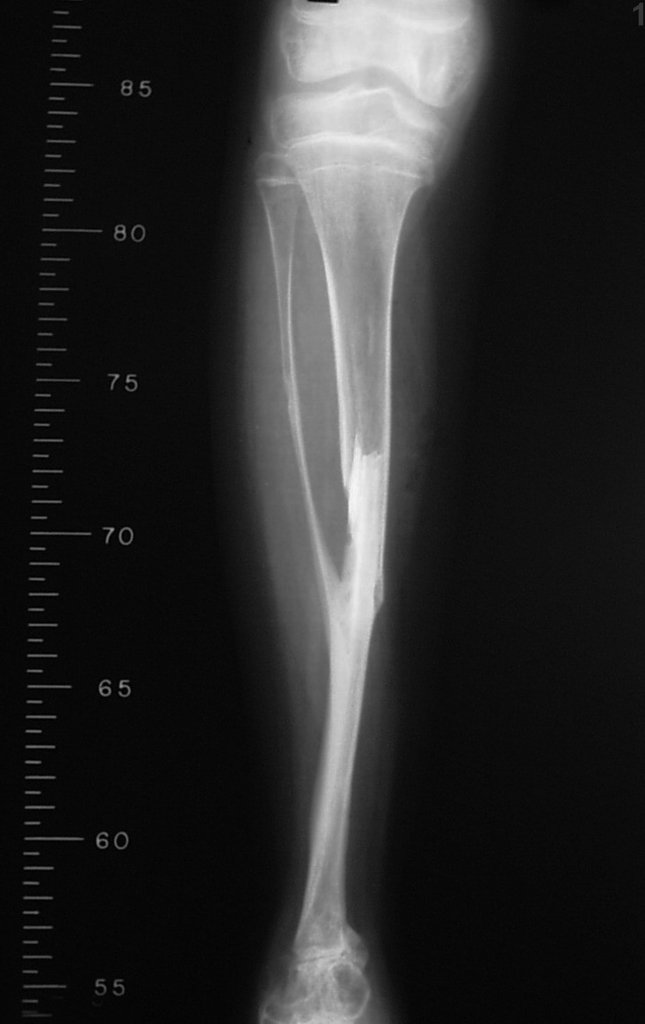
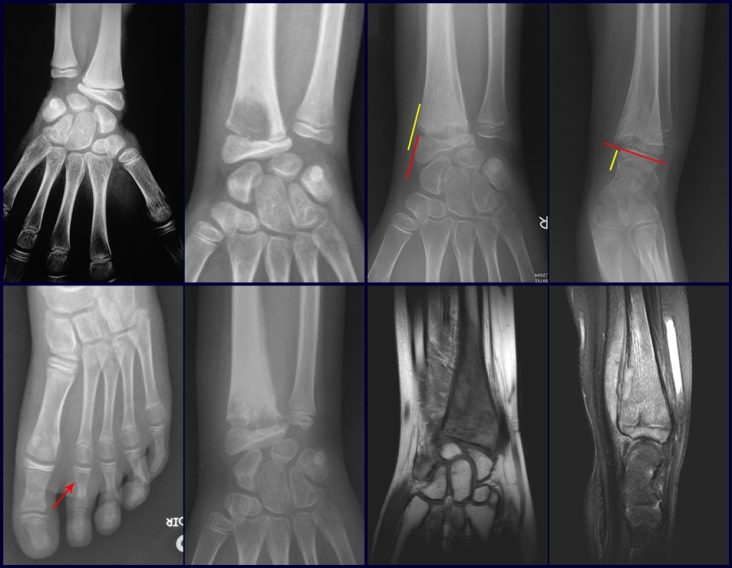
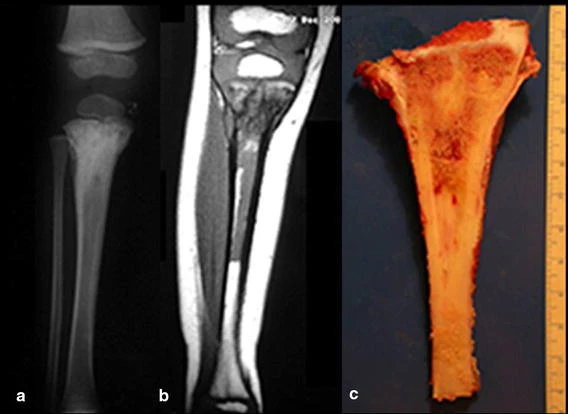
Female child, nine years and three months old, with a history of direct trauma to the right ankle two months ago, evolving with pain and local edema. She sought medical treatment and was diagnosed with a contusion. Plaster immobilization was performed for six days. Fifteen days later, she noticed an increase in volume in her ankle, which was painful and hardened, and sought our service. The radiograph revealed a radiolucent lesion, centrally located, in the distal third of the tibia, with imprecise radiographic limits and a thin laminar periosteal reaction (fig. 1). Bone scintigraphy showed intense uptake only at the site and nuclear magnetic resonance (fig. 2) showed intense involvement of the meta-epiphyseal region, with evident involvement of the tibial epiphyseal plate. Laboratory tests demonstrated changes in bone metabolism, with very high alkaline phosphatase and serum calcium. We performed a needle biopsy, and the diagnosis of chondroblastic osteosarcoma was confirmed. Neo-adjuvant chemotherapy treatment began, with three cycles of chemotherapy. As part of the pre-operative surgical planning, we performed arteriography (fig. 3) to visualize the emergence of the nutrient artery of the fibula, a time that we considered important to identify the safe site for the osteotomy and its transposition. A polyethylene cruropodal orthosis was made prior to surgery, aiming for adequate immobilization, providing better support for the limb in the postoperative period (fig. 4). After neo-adjuvant chemotherapy, she underwent surgical treatment.


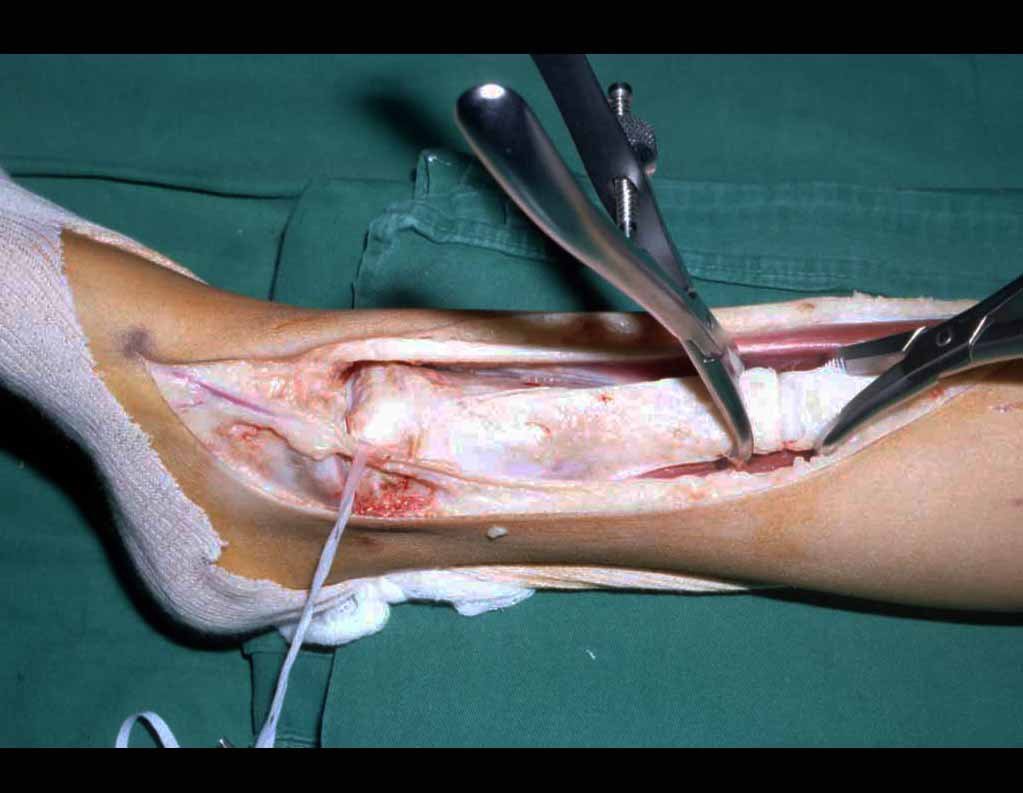
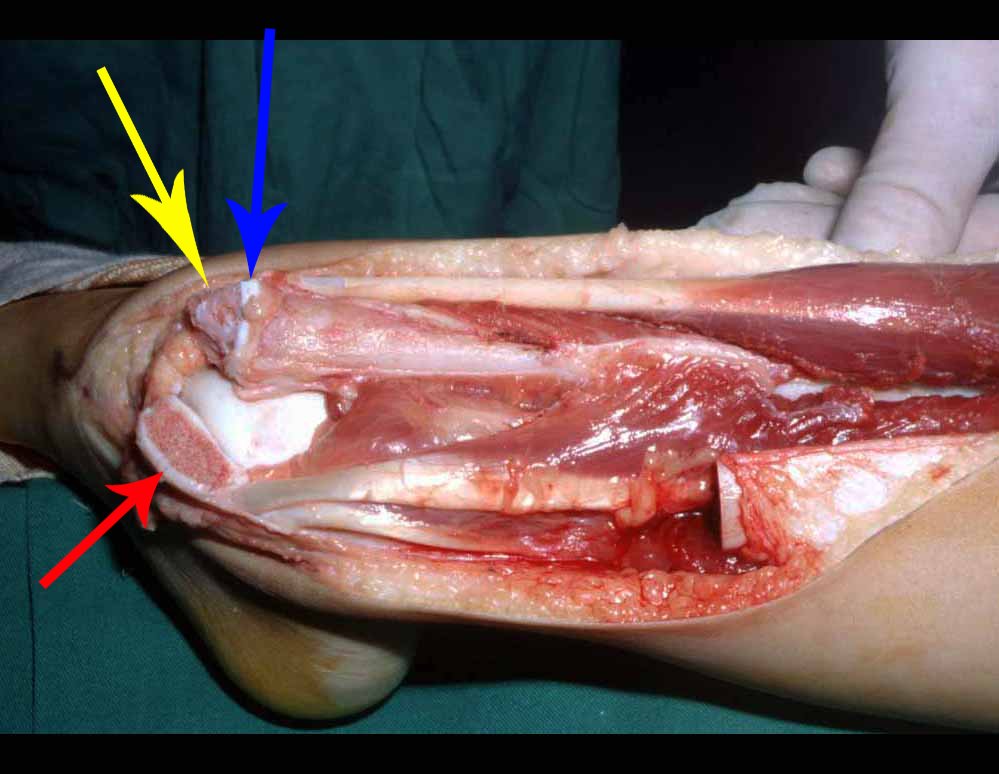
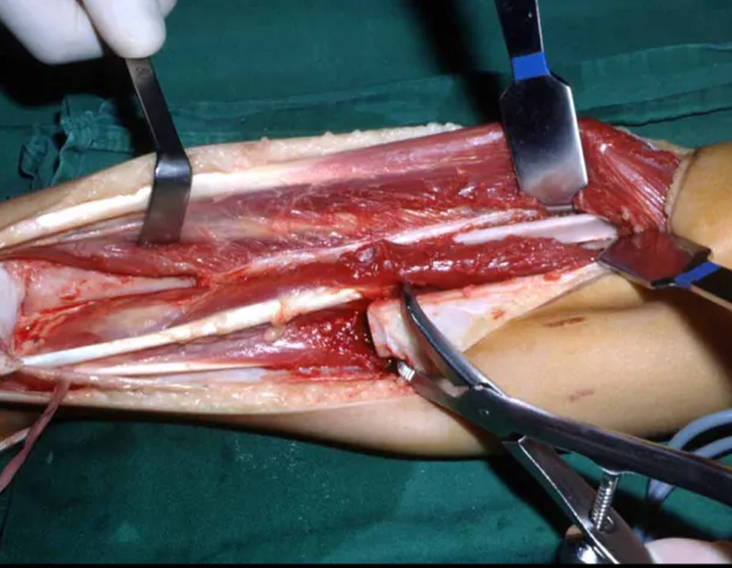
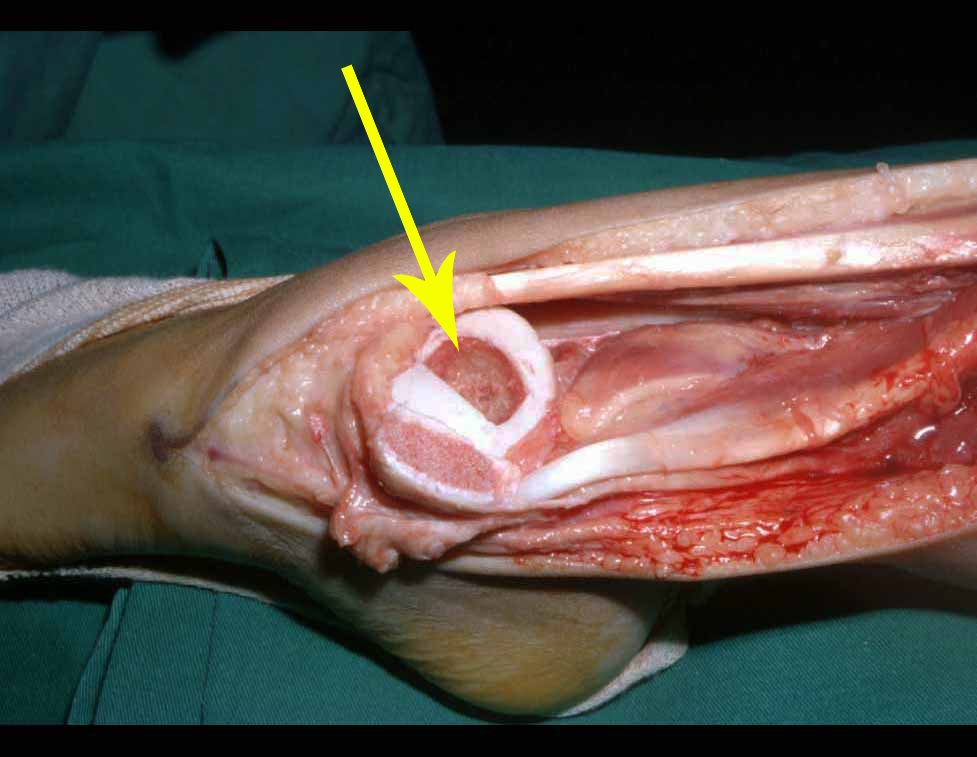
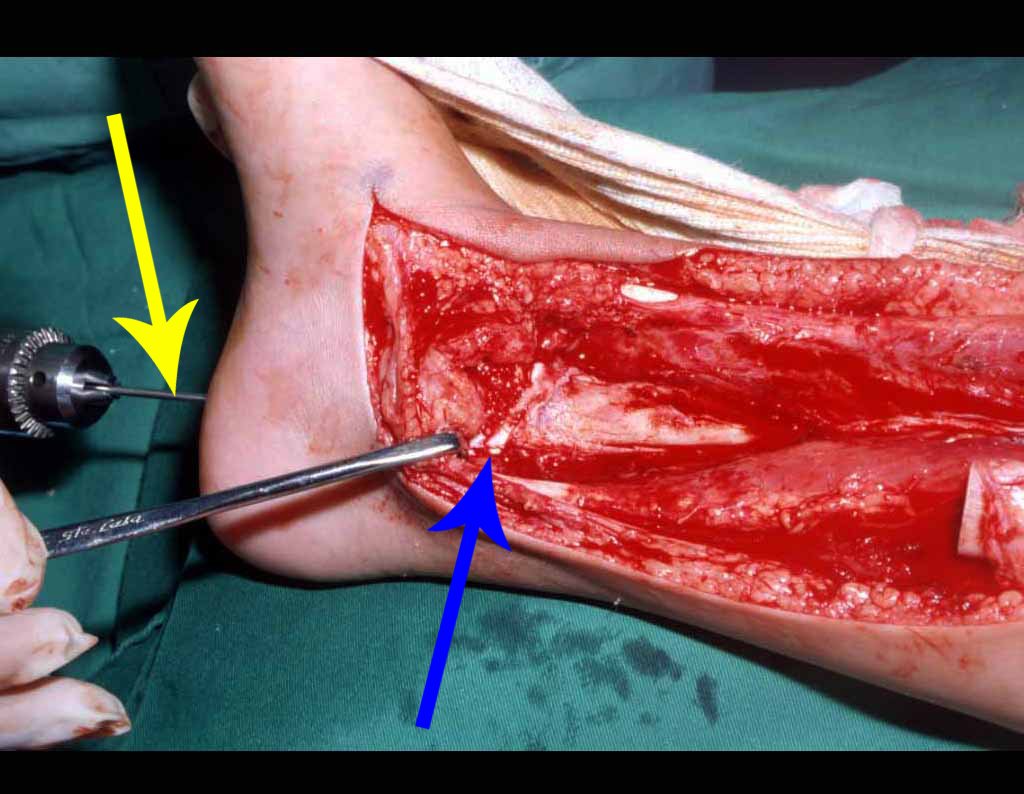
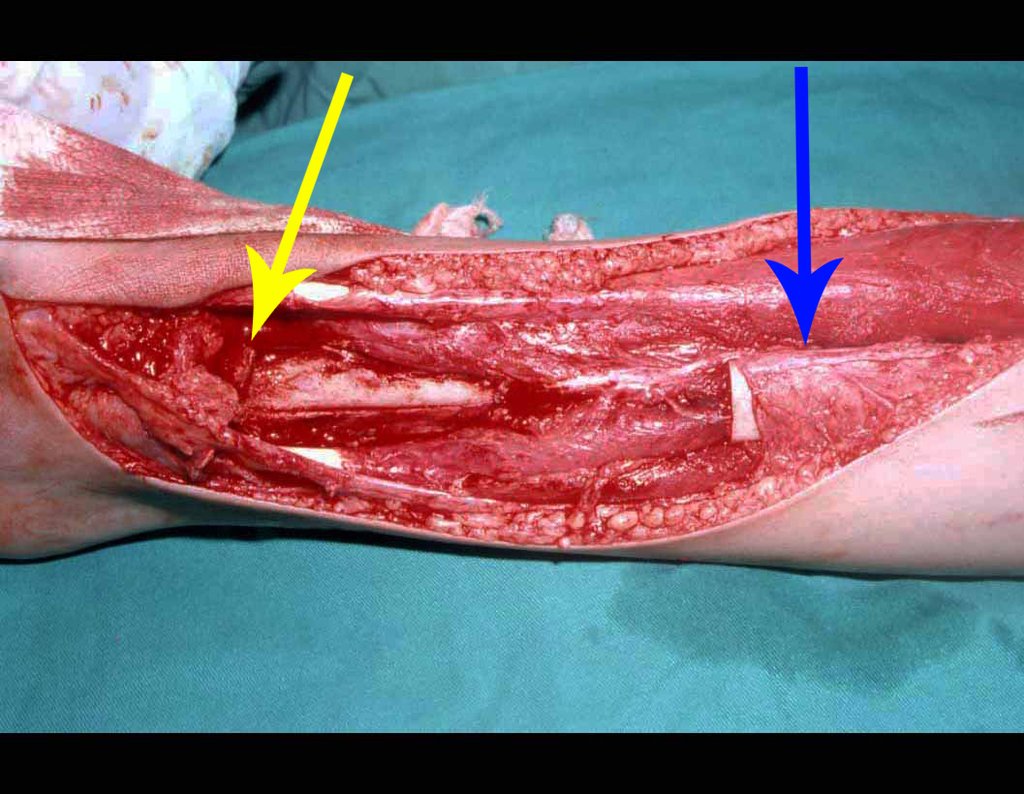
The surgery is performed with a medial convex arcuate incision starting at the level of the head of the fibula, passing through the anterior surface of the leg, up to the end of the lateral malleolus. The lesion is resected with a macroscopic oncological margin in the soft tissues and a 3.0 cm bone margin (fig. 5). After resection of the tumor, using the interosseous membrane as a guide, we approached the site of the osteotomy of the proximal fibula, above the emergence of the nutrient artery, confirmed by a previous arteriographic study (fig. 6). In this case, as the resection of the tibial segment was smaller, we opened a slit on the lateral surface of the proximal segment of the tibia, approximately 3.5 cm long and wide enough to enable its interlocking, with minimal deperiostization. from the proximal end of the transposed segment, and without harming the nutrition provided by the nutrient artery. Next, we remove the cartilage from the fibular epiphysis and carve a hole in the dome (fig. 7) of the talus, allowing this distal fibular epiphysis to fit. We continued with the careful passage of a 2.5mm diameter wire through the medullary canal of the fibula, crossing the physeal plate. This thread continues through the epiphysis and is passed through the talus and calcaneus until it appears on the skin (fig. 8).





In the immediate postoperative period, the limb was kept in immobilization with the previously made cruropodal device. Six weeks after surgery, we performed bone scintigraphy with axial sections, confirming good vascularization of the graft (fig. 11). In the metaphyseal region of the transplanted fibula, the increase in hyperuptake may be due to the vascularization of the physeal plate itself and also to the reparative process at the site of the talofibular arthrodesis. Radiographic controls from September/98, nine months after surgery, show complete integration of the transposed fibula, both proximally and distally. The thickening of the fibula is already evident and its growth plate can be easily distinguished (fig. 12).
Advances in polychemotherapy in the treatment of osteosarcoma have brought new perspectives regarding the prognosis and approach of affected patients. Controlling the disease through chemotherapy made it possible to preserve limbs, allowing new possibilities and the most varied solutions to be proposed(4,8,13). One of the solutions was the replacement of the affected segment with non-conventional internal prostheses. However, in young children, there are basically two major problems: patients continue to grow and prostheses become insufficient, making amputation necessary in some cases, often years after the start of treatment(5 .6); Furthermore, prostheses suffer excessive wear and young patients have to undergo early revisions. Prosthetics in children have very limited indications(6). With the considerable increase in survival, it became necessary for the orthopedic surgeon to look for long-lasting limb-saving surgical solutions. The use of a homologous graft to fill the bone gap is an option. However, in addition to the greater difficulty in integrating the graft, the greater number of complications, even exceeding those of endoprostheses, it also requires a bone bank, which is not always possible in our reality(6). The use of autologous grafts is sometimes limited when there is a need to replace large resections. Vascularized bone grafting has been used more frequently and presents good results. When replacing segments of the tibia, the option has been to use the ipsilateral or contralateral vascularized fibula, and several techniques have been proposed(3,5,9-12,15-18,23-25). Some of these techniques are performed in two operative stages, which increases morbidity. Microsurgical techniques are also used, but they require a specialized team, with prolonged surgical time. The technique presented here is quick, easy to perform, performed in a single surgical procedure and does not require a microsurgical technique. In an attempt to preserve the length of the limb, we transposed a segment of the fibula with the distal physis, hoping that it will remain active. We cannot yet say, due to the short follow-up period, that preservation of the physis in the fibular transposition technique will lead to bone growth, nor how this growth will occur.
The biological solution in the treatment of osteosarcoma is an increasingly common reality in our country and should always be considered. We believe that the presence of bone hyperuptake at the level of the projection of the physeal plate of the distal fibula in bone mapping exams may be evidence that it is viable, although it is impossible to distinguish how much of this process is due to bone reaction at the level of fixation of the epiphysis of the fibula in the body of the talus. Considering the short follow-up period and the fact that this is a single case, it is not possible to definitively evaluate the treatment method used. What we can say with satisfaction, at the moment, is that the radiographic controls from September/98, nine months after surgery, show complete integration of the transposed fibula, both proximally and distally. Thickening of the fibula is already evident and the fibular growth plate can be easily distinguished. We believe that growth will occur and we hope that there will be adaptation of this physeal plate, so that it grows with the speed of the tibia, as we know that the speed of growth is also influenced by the location in which it is located.
1. Bacci, G. et al: Primary chemotherapy and delayed surgery for non-metastatic telangiectasic osteosarcoma of the extremities: results in 28 patients. Eur J Cancer 30A: 620-626, 1994.
2. Campanacci, M.: “Classic osteosarcoma”, in Campanacci, M. et al: Bone and soft tissue tumors, Bologna, Aulo Gaggi Ed., 1990. p. 455-480.
3. Campbell, WC: Transference of the fibula as an adjunct to free bone graft tibial deficiency: report of three cases. J Orthop Surg 1:625, 1919.
4. Carter, SR, Grimer, RJ & Sneath, RS: A review of 13-year experience of osteosarcoma. Clin Orthop 270: 45-51, 1991.
5. Chacha, PB: Vascular pedicle graft of the ipsilateral fibula for non-union of the tibia with a large defect. J Bone Joint Surg [Br] 63: 244- 253, 1981.
6. David, A. et al: Osteosarcoma: review of 39 cases. Rev Bras Ortop 33: 45-48, 1998.
7. Davis, AM, Bell, RS & Goodwin, PJ: Prognostic factors in osteosarcoma: a critical review. J Clin Oncol 12: 423-431, 1994.
8. Dubousset, J., Missenard, G. & Kalifa, C.: Management of osteogenic sarcoma in children and adolescents. Clin Orthop 270: 52-59, 1991.
9. Girdlestone, GR & Foley, WB: Extensive loss of tibial diaphysis. Ti-bio-fibular grafting. Br J Surg 20: 467-471, 1933.
10. Hahn, E.: Eine methode, pseudoarthrosen der tibia mit grossem knochen defect zur heitung zubringen. Zentralbl Chir 11: 337-341, 1884.
11. Huntington, TW: Case of bone transfer. Ann Surg 41: 249-251, 1905.
12. Jones, KG & Barnett, HC: Cancellous bone grafting for non-union of the tibia through the posterolateral approach. J Bone Joint Surg [Am] 37: 1250-1260, 1955.
13. Lane et al.: Osteogenic sarcoma. Clin Orthop 204: 93-110, 1986.
14. Marwin, MR: Amputation for osteosarcoma. Cancer Bull 42: 337-343, 1990.
15. McCarrol, HR: The surgical management of ununited fractures of the tibia. JAMA 175: 578-583, 1961.
16. McMaster, PE & Hohl, M.: Tibiofibular cross-peg grafting. J Bone Joint Surg [Am] 47: 1146-1158, 1965.
17. Meyerding, HW: Tibial defects with non-union created by the transfer of the fibula and tibiofibular fusion. Am J Surg 52:397-404, 1941.
18. Milch, H.: Synostosis operation of persistent non-union of the tibia. A case report. J Bone Joint Surg [Am] 21: 409-420, 1939.
19. Petrilli, S. et al: IIB osteosarcoma. Current management, local control and survival statistics – São Paulo, Brazil. Clin Orthop 270: 60-66, 1991.
20. Picci et al: Relationship of chemotherapy-induced necrosis and surgical margins to local recurrence in osteosarcoma. J Clin Oncol 12: 2699-2705, 1994.
21. Simon, AM & Springfield, D.: Surgery for bone and soft tissue tumors, Baltimore, Lippincott-Raven, 1998. p. 266.
22. Spanier, SS, Shuster, JJ & Griend, RAV: The effect of local extent of the tumor on prognosis in osteosarcoma. J Bone Joint Surg [Am] 72: 643-653, 1990.
23. Stone, JS: Partial loss of the tibial replaced by transfer of the fibula, with maintenance of both malleoli of the ankle. Ann Surg 46: 628-632, 1907.
24. Taylor, GI & Millar, GDH: The free vascularized bone graft, a clinical extension of microvascular techniques. Plast Reconstr Surg 55: 533-544, 1975.
25. Wilson, PO: A simple method of two-stage transplantation of the fibula for use in cases of complicated and congenital pseudoarthrosis of the tibia. J Bone Joint Surg [Am] 23: 639-675, 1941.
Click here to download the PDF
Click here to see the complete technique in more detail.
Use of extensible internal device in the femur of young dogs .
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com
Farber and Green, in 1942, demonstrated that the lesion could occur in a localized or multiple manner in the skeleton and possibly be related to Hand-Schuller-Christian disease and Letter-Siwe disease3.
In 1944, Jaffe and Lichtenstein introduced the term eosinophilic granuloma of bone4. The relationship of this lesion with the systemic forms of the disease was confirmed by Lichtenstein in his 1953 publication, encompassing them under the name Histiocytosis X5.
Currently, this entity is called Langerhans Cell Histiocytosis, which has four distinct clinical forms: Eosinophilic Granuloma, a form restricted to the skeleton, which can be localized or multiple; Hand-Schuller-Christian, chronic and disseminated form; Letter-Siwe, acute or subacute disseminated form and Hashimoto-Pritzker, postnatal form with spontaneous resolution6.
Introduction: Solitary eosinophilic granuloma of the bone is the most common of the four forms of presentation of Langerhans Cell Histiocytosis, representing between 60% and 80% of cases7.
Among benign bone lesions, it is a rare entity, accounting for less than 1%8. It preferentially affects children and adolescents with a male predominance 2:19. Around 80% of patients are under 21 years of age and the majority of these are between five and 15 years of age6,7,9.
Some patients may begin with an isolated bone lesion and later develop multiple bone lesions. These cases can eventually evolve into systemic forms of the disease. When this occurs, it generally happens within the first six months of diagnosis and practically never after a year of evolution, which is a criterion for good prognosis, when no new lesions appear after this period of clinical follow-up10.
Hand-Schuller-Christian Syndrome is the chronic form of Langerhans cell histiocytosis, characterized by systemic involvement with multiple bone lesions, mainly in the skull, exophthalmos and diabetes insipidus, affecting children over 3 years of age10.
Letter-Siwe Syndrome affects children under three years of age, it is the acute or subacute form, also with systemic involvement. It presents with fever, otitis media, recurrent bacterial infections, anemia, hemorrhages, viceromegaly, diffuse and painful adenopathy with skin involvement similar to seborrheic eczema and generalized ostelitic lesions, with frequent progression to death10.
Hashimoto-Pritzker Syndrome is a form of Langerhans cell histiocytosis that affects the skin exclusively. It affects children in the first month of life, manifesting with eczematous eruptions that resolve spontaneously6.
Etiology: Unknown.
Genetics: No significant reports regarding this.
Definition: Eosinophilic Granuloma is a pseudotumor lesion, of unknown etiology, characterized by bone rarefaction that can be solitary or multiple. Microscopically, it presents a profile of mononuclear histiocytic cells, presenting antigens of dendritic origin, known as Langerhans cells, amidst the variable quantity of leukocytes, eosinophils, lymphocytes and giant cells.
Epidemiology: Eosinophilic Granuloma mainly affects the axial skeleton, in this order: skull, pelvis, vertebrae, ribs, mandible, clavicle and scapula.
In the appendicular skeleton the femur, proximal region and diaphysis, humerus and tibia9. Most of the time it affects the diaphysis or metadiaphyseal region, being rare in the epiphysis7.
The spine represents 10% of cases in the pediatric population, the majority in the lumbar region.
In adults, it occurs more frequently in the ribs and less frequently in the spine, respectively 25% and 3%6.
Clinical picture: The most frequent symptom of Eosinophilic Granuloma is localized, throbbing, short-lasting pain, worsening at night associated with local heat and edema. When it affects the skull, this pain can be confused with other causes of headache.
Compromise of vertebral bodies can produce painful scoliosis. Any angular deviations are small, less than 100, as the vertebral flattening is usually uniform and rarely produces neurological symptoms.
In other forms of Langerhans Cell Histiocytosis, systemic symptoms may be present such as fever, skin rush and diabetes insipidus. Hepatosplenomegaly can occur in Letter-Siwe syndrome, which is the most severe form of the disease6
Classification: Eosinophilic granuloma can manifest itself in two clinical forms: Solitary or Multiple .
Laboratory tests: Laboratory changes that can be found are an increase in ESR and CRP, and mild eosinophilia may occasionally occur in the blood count.
Imaging tests: The radiographic image is of bone rarefaction, rounded or oval, which begins in the medullary bone and progresses with erosion of the cortical bone.
In the initial phase, the edges are irregular and poorly defined.
In the late phase, slight sclerosis may occur around the lesion. In long bones, there is an evident periosteal reaction that appears as multiple thick lamellar layers, which characterizes slow-evolving benign lesions or the reaction of osteomyelitis.
This type of solid periosteal reaction differentiates Eosinophilic Granuloma from Ewing’s Sarcoma, where the periosteal reaction is thin lamellar, due to the rapid evolution of the malignant tumor.
Another radiographic difference between these two lesions is that Ewing’s tumor early presents extra-cortical tumor tissue, with a large volume, which does not occur in Eosinophilic Granuloma.
In flat bones, such as the skull or pelvis, erosion affects both cortices in an irregular and asymmetrical manner, producing the visual impression of a hole within another hole, called a double contour lesion.
In the mandible, destruction of the alveolar bone produces the radiographic impression of floating teeth.
In the spine, the disease affects the vertebral body, with flattening occurring in 15% of cases, producing the so-called flat vertebra of Calvè6. The posterior elements and intervertebral discs are preserved, even when the injury occurs in more than one vertebra.
Pathologic anatomy:
Macroscopic appearance: it has a soft, gelatinous consistency, yellowish in color, necrotic liquefaction is common.
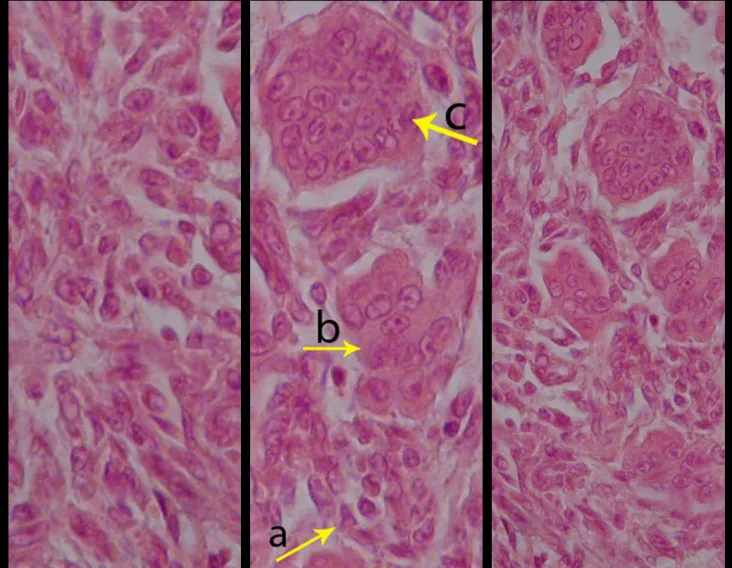
Microscopic appearance: They appear as clusters of large histiocytic cells, with a slightly basophilic cytoplasm, globose, lobulated or indented nucleoli, in these cases similar to a bean seed, which correspond to Langerhans cells.
These clusters are interspersed with giant cells, lymphocytes, numerous eosinophils and areas of necrosis, simulating an abscess. Electron microscopy presents typical cytoplasmic granules called Birbeck bodies11,12.
Immunohistochemistry shows positivity for S-100 protein, vimentin and CD1a11,13.
Diagnosis:
Differential diagnosis: The main radiological differential diagnoses of Eosinophilic Granuloma are Osteomyelitis and Ewing Tumor.
When the lesion occurs in the skull, it must be differentiated from an epidermoid cyst or metastasis. The main histological differential diagnoses are Osteomyelitis and Lymphoma.
Staging:
Treatment: The literature presents reports that expectant treatment or biopsy alone can be indicated as an effective therapeutic strategy for isolated skeletal injuries7,14.
Eosionophilic Granuloma can resolve spontaneously, especially in children. The capacity for the affected bone to rebuild itself exists, as the majority of patients are affected before skeletal maturity, therefore with great potential for remodeling by the growth physes, which are normally not affected15,16.
In our experience, there was resolution in five cases, which regressed only with percutaneous biopsy. The same happens after vertebral collapse in spinal injuries, probably due to the leakage of the contents of the lesion, resembling the drainage of an abscess, with surgical indication in the spine being extremely rare. Cases have been reported where there was complete restitution of the height of the vertebral body15. In our series we had two cases that presented this evolution.
Although there may be spontaneous resolution, the time required is unpredictable, and there may be significant morbidity secondary to intense pain and functional limitation.
Currently, the best therapeutic approach for Eosionophilic Granuloma is to perform a percutaneous biopsy, if possible with immediate diagnosis by frozen section, followed by intralesional corticosteroid infusion (methylpredinisolone – 40mg to 120mg depending on the size of the lesion)7. The anatomopathological result must be subsequently confirmed by histology in paraffin blocks.
Eosionophilic Granuloma can take up to three months to regress, and it may be necessary to repeat the infusion6. In our experience, we had only one case, of an isolated injury to the humerus, which required complementation of the initial treatment in which we performed oral corticosteroid therapy, prednisolone 5mg/24h, for four months. In polyostotic Eosinophilic Granuloma, systemic corticosteroid therapy is used.
When an incisional biopsy is necessary, corticosteroids can be applied locally after curettage of the lesion, which facilitates the resolution of the process. This curettage must be careful, carried out by opening in the form of a narrow slit, longitudinal to the bone, trying not to add greater local fragility. Eventually, the cavity can be filled with a bone graft, but this is generally unnecessary due to the great potential for regeneration that exists.
Radiofrequency was proposed as a percutaneous treatment for Eosionophilic Granuloma, being applied in a second stage, two to four weeks after the biopsy17. The author restricts the technique to small injuries that are at least one centimeter away from the neural or visceral structures, warning of the risk of fractures in the load-bearing limbs. This approach, in addition to increasing costs and causing local morbidity, does not add any advantage to the treatment. The biopsy itself may have been curative, and the infusion of corticosteroids has greater justification, as this is indicated both in isolated cases and in multiple lesions. To date, there are no studies comparing percutaneous techniques with corticosteroid infusion in relation to the use of radiofrequency that justify their use.
Historically, radiotherapy was used in low and fractionated doses for the treatment of Langerhans Cell Histiocytosis. Currently, the indication of radiotherapy for benign lesions is controversial.
In cases of eosinophilic granuloma with more than one skeletal lesion, without visceral involvement, systemic treatment may be indicated for a period of approximately six weeks with corticosteroid therapy (2 mg/kg) and Vinblastine (6 mg/kg).
Prognosis: Solitary lesions of eosinophilic granuloma evolve well in 97% of cases, with biopsy alone or in addition to corticosteroid infusion or surgical treatment 6 .
See also: Eosinophilic granuloma of the radius
Bibliography:
1 SCHAIRER, E. Ueber eine eigenartige Erkrankung des kindlichen Schädels. Zentralbl Allg Patho Pathol. Anat., 71:113, 1938.
2 Otani S, Ehrlich JC; Solitary granuloma of bone simulating primary neoplasm. Am J Pathol 16:479–90. 1940
3 Green WT, Faber S; “eosinophilic or solitary granuloma” of bone. J Bone Joint Surg (Am) 24:499-526. 1942
4 Jaffe HL, Lichtenstein L; Eosinophilic granuloma of bone. Arch Pathol 37: 99-118. 1944.
5 Lichtenstein L.: Histiocytosis Pathol. 56:84, 1953
6 Schwartz HS. Orthopedic Knowledge Update: Musculoskeletal Tumors 2. American Academy of orthopedic Surgeons, Rosemont, Illinois. Chapter 12 (128-32), 2007
7 Mavrogenis AF, Abati CN, Bosco G, Ruggieri P. Intralesional Methylprednisolone for Painful Solitary Eosinophilic Granuloma of the Appendicular Skeleton in Children. J PediatrOrthop 2012;32:416–422
8 Chadha M, Agarwal A, Agarwal N, et al. Solitary eosinophilic granuloma of the radius. An unusual differential diagnosis. Acta Orthop Belg. 2007; 73:413–417.
9 Campanacci, M. Bone and Soft Tissue Tumors; Springer-Verlag Wien New York. Second Edition, (54); 857-75. 1999.
10 SCHAJOWICZ, F. Buenos Aires: Osseous Tumors; Talleres de editorial Médica Panamericana SA (9); 464-80. 1981.
11 CHRISTIAN, HA Defects in membranous bones, exosphthalmos and diabetes insipidus: in a usual syndrome of dyspituitarism: a clinical study. Med.Clin. North. Am., 3:849, 1920.
12 ARCECI, RJ; BRENNER, M.K.; PRITCHARD, J. Controversies and new approaches to the treatment of Langerhans cell histiocytosis. Hemtol. Oncol. Clinic. North. Am., 12:339, 1998
13 ALBRIGHT, F.; REIFNSTEIN, EC The parathyroid glands and metabolic disease. Baltmore, Williams & Wilkins, 1948.
14 Plasschaert F, Craig C, Bell R, et al. Eosinophilic granuloma. A different behavior in children than in adults. J Bone Joint Surg Br 2002;84:870–872.
15 Greenlee JD, Fenoy AJ, Donovan KA, et al. Eosinophilic granuloma in the pediatric spine. Pediatr Neurosurg. 2007; 43:285–292.
16 Sessa S, Sommelet D, Lascombes P, et al. Treatment of Langerhans cell histiocytosis in children. Experience at the Children’s Hospital of Nancy. J Bone Joint Surg Am. 1994; 76:1513–1525.
17 Corby RR, Stacy GS, Peabody TD, et al. Radiofrequency ablation of solitary eosinophilic granuloma of bone. Am J Roentgenol.2008;190:1492–1494.
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com

a Department of Orthopedics, Santa Casa de São Paulo, São Paulo, SP, Brazil
b Orthopedics and Traumatology Service, Hospital Israelita Albert Einstein, Federal University of São Paulo (Unifesp), São Paulo, SP, Brazil
c Institute of Orthopedics, Hospital das Clínicas, Faculty of Medicine, University of São Paulo (USP), São Paulo, SP, Brazil
d Escola Paulista de Medicina, Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil
Introduction
Damage control in orthopedics is a surgical tactic recommended for polytraumatized patients or those with severe soft tissue injuries, as recognized in the literature.1However, this procedure is not without risks. Local and systemic complications associated with external fixation for damage control2 have been reported, and one of them is bone infection. Studies show infection rates in pin tracts ranging from 0.5 to 30%.
Bacterial contamination and infection in the path of external fixator pins are relatively common and conversion to internal osteosynthesis, whether with intramedullary nails or plates, in the presence of such a condition, can lead to serious complications, local and/or systemic.4The frequency of this association of events is not clear in the literature.
The correlation between infection in the path of external fixator pins and post-traumatic osteomyelitis after internal osteosynthesis, which constitutes chronic infection of the locomotor system, is well established.
Infection at the bone-fixator pin interface has been proven to be directly associated with the insertion technique, stability and position in the limb, during pin placement, by establishing tension or not in the soft parts. The presence of these factors contributes to infectious complications after conversion to definitive internal osteosynthesis, whether intramedullary nail or plate.
The objective of our work is to identify in patients undergoing control of musculoskeletal damage admitted to the emergency room for one year, the quality of reduction and fixation and the frequency of bone infection after definitive treatment.
Casuistry and methods
This work was duly submitted to and approved by the institution’s Ethics Committee and is registered under protocol CEP no. 624.307.
We retrospectively evaluated 120 patients who underwent external fixation to control musculoskeletal damage from June 2012 to June 2013 and were treated at the time of emergency in the emergency room of the Department of Orthopedics and Traumatology at our institution.
In this retrospective study, we included patients who underwent damage control surgery using external fixation that
after conversion to definitive osteosynthesis, they developed infection.
Patients who presented infectious complications due to local systemic changes, such as vasculopathies, diabetes mellitus or consumptive disease, and patients with psychiatric disorders that may have impaired the development or care of the fixator in any way were excluded.
All radiographs were generated in digital form and analyzed using the Impax program. The distances between Schanz holes and pins until the definitive synthesis were analyzed in the program itself. We sought to identify the presence of technical errors during drilling (characterized by multiple perforations) or subjective analysis carried out by three different groups of two evaluators. One group was made up of assistant doctors with at least five years of experience in orthopedic trauma, another with two third-year residents and another with two second-year orthopedic residents. The evaluators were named (table 1):

– Evaluator 1: assistant with more than five years of experience
– Evaluator 2: assistant with more than five years of experience
– Evaluator 3: third year resident
– Evaluator 4: third year resident
– Evaluator 5: second year resident
– Evaluator 6: second year resident
Postoperative infection was characterized by clinical examination, during hospitalization or during outpatient investigation, based on data recorded in the medical records. The following clinical criteria for infection were considered: erythema, hyperemia or fistula in the path of the pins or surgical incision (fig. 1).
During external fixation, prior drilling with a drill and manual insertion of the pins were always respected.

In no case did we have a pin in the fracture exposure zone.
In evaluating the radiographs, we observed the pre- and post-operative exams, we measured the position and distance of the Schanz pins in relation to the definitive synthesis, the presence of perforations in a greater number than the pins installed as this suggests difficulty and additional damage in installing the external fixator, presence of osteolysis in the holes for the Schanz pins and if the place where the pins were drilled caused problems for definitive internal fixation. Among these, we evidence postponed surgery due to infection in the pin path, changes in the surgical incision for definitive osteosynthesis and unplanned surgical procedures for reassembly of the fixator due to unstable assembly.
The average conversion time from external fixators to definitive osteosynthesis was evaluated by retrospective analysis of medical records.
Results
Of the 120 patients who underwent damage control, 16 (13.3%) suffered post-traumatic osteomyelitis after definitive synthesis. In these 16 patients, we were able to directly relate it to definitive internal osteosynthesis, as there were no signs of local infection after external fixation in the urgency.
The average age of these 16 patients was 43.4 years, ranging from 19 to 81. We observed a predominance of males, with 13 patients (81.2%), and the remaining three (18.8%) females.
Regarding the external fixator conversion time for definitive osteosynthesis, the shortest period was five days and the longest was 30. We had an average of 15 days for the final conversion.
Infection occurred in eight isolated leg fractures (50%), two patients with fractures of the femur and ipsilateral tibia (floating knee), two (12.5%) with ankle fractures (12.5%), two (12.5%) %) with a tibial plateau fracture, one (6.2%) with an isolated femur fracture and one (6.2%) with a humeral fracture.
Of the 16 patients with post-traumatic infection, 37.5% of the time (six patients) occurred after closed fractures and in 62.5% (10) after Gustillo grade 3 A open fractures (table 2).
In 62.5% (10 patients) the fixator was mounted transarticularly and in the remaining six (37.5%) it was monostolic with monolateral configuration, with tube-to-tube connection.
As for the etiological agent, it was adequately identified in 10 patients (62.5%) of the 16 infected, in a third of these there were multiple bacteria and there was a need for surgery to clean, debridement and curettage of the pin hole path. The polymicrobial findings found in intraoperative cultures were: Staphylococcus aureus, coagulase-negative Staphylococcus, Klebsiella sp, Acinetobacterbaumanni and Pseudomonas aeruginosa.
Regarding the objective assessment of multiple bone perforations, we observed a greater number than pins used in eight patients (50%) of the 16 patients infected after definitive osteosynthesis (fig. 2).

When we measured the distance between the position of the Schanz pin and that of the osteosynthesis, we obtained an average of 2.2 cm, with a variation of up to 6 cm. In seven cases (43.8%) of the 16 infected people, the distance measured was 0 cm, two between 1 and 2 cm, two between 3 and 4 cm, one between 4 and 5 cm, three with 5 cm and one with 6 cm (table 2). Regarding the evaluation of the quality of fixation and reduction, we were able to observe that of the 16 cases, in four (25%) the six evaluators agreed, in two the fixation was considered adequate and in the other two inadequate; in five cases (31.3%) five evaluators agreed on the quality of the evaluation, in two it was considered adequate and in three inadequate; in four cases (25%) four evaluators agreed with the evaluation, all were considered inadequate; In three cases (18.7%) there was no agreement between the evaluators, three considered the fixation and reduction to be adequate and three others to be inadequate (table 3).
In the 13 cases (81.2%) in which there was some agreement (adequate or inadequate), it was considered adequate in four (30.8%) and inadequate in nine (69.2%).
When analyzing the evaluations, we obtained 96 evaluations, which were considered adequate in 38 cases (39.6%) and inadequate in 58 cases (60.4%). When analyzing the evaluations of each evaluator, we obtained for evaluator one: five cases (31.3%) evaluated as adequate and 11 (68.7%) as inadequate; assessor two: 10 cases
When we separately evaluated orthopedists with more than five years of experience, we obtained 32 evaluations, 15 (46.9%) were considered adequate and 17 (53.1%) were considered inadequate (table 4). In this group, there was agreement in the quality of fixation and reduction in nine cases (56.3%) and non-agreement in the remaining seven (43.7%), of the nine cases with agreement in four (44.4%). ) the quality of reduction and fixation was considered adequate and in five (55.6%) inadequate.
When we evaluated third-year residents separately, we obtained 32 evaluations, 14 evaluations (43.7%) were considered adequate and 18 (56.3%) were considered inadequate (table 4). In this group, there was agreement on the quality of reduction and fixation in nine cases (56 .3%) and non-agreement in the remaining seven (43.7%), of the nine cases with agreement in four (44.4%) the reduction and fixation was considered adequate and in five (55.6%) inadequate.
When we evaluated second-year residents separately, we obtained 32 evaluations, nine (28.1%) were considered adequate and 23 (71.9%) were considered inadequate (table 4). In this group, there was agreement on the quality of reduction and fixation in 13 cases (81.3%) and non-agreement in the remaining three (18.7%), of the 13 cases with agreement in three (23.1%), reduction and fixation were considered adequate and in 10 (76.9%) inadequate.
When observing the assessments considered adequate, we can see a tendency towards similar assessments between assistants and third-year residents, but a lower assessment of cases considered suitable for second-year residents (table 5).
When we compared the cases in which the assistants agreed with the third-year residents’ assessment, we observed that there was agreement in five (31.3%) of the 16 cases, in three the reduction and fixation was considered adequate and in two inadequate. Of the remaining 11 cases, in four, despite the agreement of the assistants’ assessment, there was no agreement with the third-year residents; in one case, the reduction and fixation was considered adequate by the assistants and in three cases, inadequate.
When we compared the cases in which the assistants agreed with the assessment of the second-year residents, we observed that there was agreement in seven (77.8%) of the nine cases, in two of these the reduction and fixation was considered adequate and in five inadequate. In one case where there was agreement from the assistants (considered adequate) the second year residents considered it inadequate.
When evaluating the seven cases in which there was no agreement among assistants with more than five years of experience, we observed that in one case the residents, whether third or second year, also did not agree. In four cases, the two third-year resident evaluators also did not agree and in three cases the two third-year resident evaluators agreed and considered the reduction and fixation inadequate. Of the seven cases in which the assistants did not agree, the second-year resident evaluators considered the reduction and fixation adequate in one case and inadequate in four.
Discussion
External fixators, more versatile fixation devices that allow different types of assemblies and configurations, can be placed quickly, are applied in the treatment of fractures in urgent and emergency situations (damage control) and in a percutaneous, with less damage to soft tissues.
This procedure, both provisional and definitive, is still routine in many services and varies from 32 to 89% of the choice of a group of orthopedists in a previous study.9However, this procedure is not without risks.
In our sample, we found a frequency of 13.3% of infection after the use of an external fixator for damage control. Although compatible with literature data, which range from 0.5 to 30%,2,3 we are concerned with judging this rate very high among the possible complications.
The first issue always remembered when searching for the etiology of the infection is the environment in which the treatment takes place, in our case a teaching hospital. It seems like a weak cause-and-effect correlation, because the procedure is considered to be of little complexity and there was at least one doctor with three years of training on the surgical team.
Another factor that is involved in the complication of infection after internal osteosynthesis is infection of the Schanz pin tract. In our patients, the presence of clinical suspicion of infection was an indication to exchange the pin for installation in another location or to continue treatment with osteosynthesis using the external fixator.
Reduction and fixation were considered inadequate in 60% of evaluations, a value considered very high, and on average, assistants and third-year residents found reduction and fixation adequate in only 50% of evaluations. This shows that there is a need for better teaching in the treatment of emergency situations with external fixators.
External fixation is often neglected in our environment both in its preoperative planning, procedure and subsequent care. In any external fixation procedure, the future definitive synthesis must always be considered when assembling the fixator and placing the pins. This situation should always be discussed with the attending physician, who can make a pre-operative schedule with a view to future synthesis, whether plate or rod. In our study, in 43.8% of cases, the location of the Schanz pin was not far from the definitive osteosynthesis.
The correct technique for inserting the pin, care with the dressing and the surgical wound are essential to prevent these complications.9,10Pre-drilling, manual insertion of the pins, use of the safety corridor are factors that cannot be forgotten during the fixation. The systematization of this intra- and post-operative care is a factor that we found capable of control by the doctor to influence the infection rate of the Schanz pin path in damage control.
Routinely, the quality of fracture reduction is not so important to consider postoperative infection, since the use of the external fixator is temporary.8 However, in some situations in which the fixator remains in place for a prolonged time, this factor must be taken into account. In our series, the longest period for conversion was 30 days and the temporary reduction is important for stabilizing the condition, local care and general condition.
In our cases, we observed that all of them had a safety event respected in the analysis of the radiographs (in our case series, no neurovascular lesions were observed).
When we identified the importance of the quality of the installation and spatial assembly of external fixators, we asked doctors with different training periods to judge the quality of the assembly and look for signs of technical inadequacy in the x-rays in the files, which occurred 60% of the time in our study, value considered very high.
Regarding the frequency of bone infection post-damage control, we confirmed that of the 13% infected, 50% identified the presence of error or technical inadequacy that may have contributed to the undesirable outcome./p>
When considering external fixator assemblies, we cannot correlate the frequency of infection with a given type of assemblage. There was a prevalence of transarticular assemblies, used in metaepiphyseal fractures, ipsilateral bone fractures and extensive soft tissue injuries to avoid post-traumatic joint deformities (62.5% of cases).
Although it was not possible to correlate infection after internal osteosynthesis and the use of fixators to control damage, the presence of inadequacy in assemblies in the emergency room suggests the possibility and need for training and rules for their use and assembly.
Conclusion
Bone infection occurred in 13.3% of cases treated with control of musculoskeletal damage after internal osteosynthesis. In these cases, reduction and fixation was considered adequate in 39.6% of evaluations and inadequate in 60.4%. We emphasize that this procedure is not without risk and training for doctors who perform it must be mandatory.
Interest conflicts
The authors declare no conflicts of interest.
Interest conflicts
The authors declare no conflicts of interest.
1. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN. External fixation as a bridge to intramedullarynailing for patients with multiple injuries and with femurfractures: damage control orthopedics. J Trauma.2000;48(4):613-21.2. Parameswaran AD, Roberts CS, Seligson D, Voor M. Pin tract infection with contemporary external fixation: how much of a problem? J Orthop Trauma. 2003;17(7):503-7.3. Mahan J, Seligson D, Henry SL, Hynes P, Dobbins J. Factors in pin tract infections. Orthopedics. 1991;14(3):305-8.4. Harwood PJ, Giannoudis PV, Probst C, Krettek C, Pape HC. The risk of local infectious complications after damage control procedures for femoral shaft fracture. J Orthop Trauma.2006;20(3):181-9.5. Green SA, Ripley MJ. Chronic osteomyelitis in pin tracks. JBone Joint Surg Am. 1984;66(7):1092-8.6. Clasper JC, Cannon LB, Stapley SA, Taylor VM, Watkins PE.Fluid accumulation and the rapid spread of bacteria in the pathogenesis of external fixator pin track infection. Injury.2001;32(5):377-81.7. Moroni A, Vannini F, Mosca M, Giannini S. State of the art review: techniques to avoid pin loosening and infection in external fixation. J Orthop Trauma. 2002;16(3):189-95.8. Cardozo RT, Silva LG, Bragante LA, Rocha MA. Treatment of tibial shaft fractures with an external fixator compared to a locked intramedullary nail. Rev Bras Ortop.2013;48(2):137-44.9. Balbachevsky D, Belloti JC, Martins CVE, Fernandes HJA, Faloppa F, Reis FB. How are open tibial fractures treated in Brazil? Cross-sectional study. Acta Ortop Bras.2005;13(5):229-32.10. Petinne KA, Chao EY, Kelly PJ. Analysis of the external fixatorpin-bone interface. Clin Orthop Relat Res 1993;293:18-27.
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com
Breast cancer is a neoplasm that most frequently originates from the excretory ducts of the gland and also from its acini. It occupies a prominent place as a cause
of death in women, but in men it is very rare. For every 100 cases of breast cancer, only one is male. It affects the adult age group, generally over 50 years old. Due to the scarcity of breast parenchyma in men, cancer infiltrates more quickly and adheres to the skin with ulceration(3,5). It behaves exactly as in invasive ductal carcinomas in women, but generally presents with minor desmoplasia. The spread is the same as in women, with
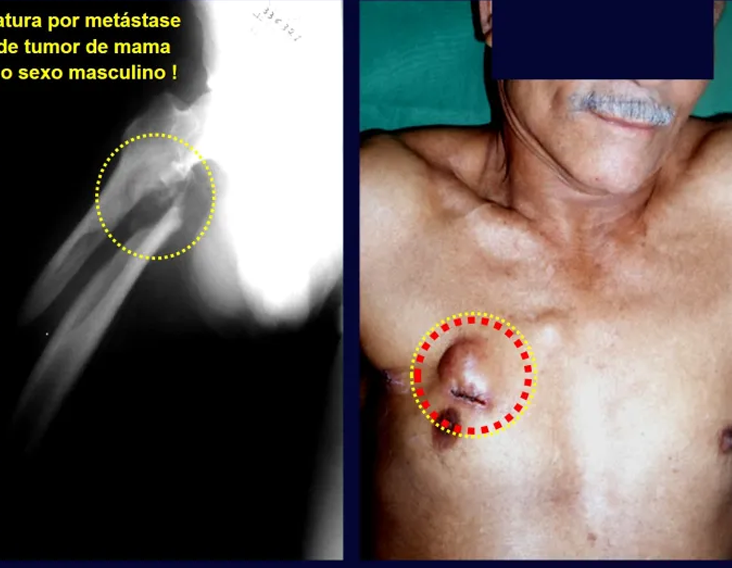
early metastases in the axillary nodes. Metastases in the lungs, brain, bones and liver are also frequent, via the hematogenous route. The femur is the most affected bone(3). The objective of this work is to report a rare case of bone metastasis from male breast carcinoma, due to its rarity and propensity for misdiagnosis.
A 69-year-old male patient was admitted to the emergency room of the Department of Orthopedics and Traumatology of Santa Casa de São Paulo, with a history of
falling to the ground four hours ago, with pain and functional impotence of the right lower limb. At admission, shortening and deformity in external rotation of the right lower limb were observed
. At the time, no other abnormalities were noted on physical examination.
On radiographic examination, in the anteroposterior projection of the pelvis and lateral aspect of the right hip (Fig. 1), a long oblique fracture without comminution or other bone injury was observed in the subtrochanteric region of the right femur. Biochemical and hematological blood analyses, chest x-rays and electrocardiogram were normal. The patient underwent anatomical reduction and osteosynthesis of the fracture with a 95º angled plate (fig. 2).


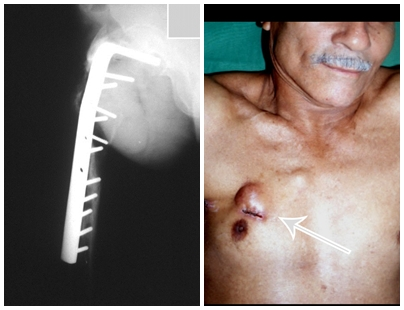
The patient underwent a trocar biopsy of the lesion in the femur and an incisional biopsy of the mass in the breast. The results of the anatomopathological examinations were as follows: metastasis of adenocarcinoma in the femur and infiltrative ductal carcinoma of the breast. A resection of the proximal third of the right femur was performed and a non-conventional Fabroni endoprosthesis (ENCF) was placed (fig. 6). The evolution in the immediate postoperative period was satisfactory. Two weeks after surgery, the patient began chemotherapy with cyclophosphamide, fluoracil and farmorubicin with the aim of facilitating breast resection and lymph node emptying. Currently (six months post-operatively), the patient, still undergoing chemotherapy, has a limp with the aid of crutches, a normal neurological examination and the following mobility of the right hip: 90º of flexion,
–15º of extension, 30º of abduction , 20º of adduction, 60º of external rotation and 0º of internal rotation (fig. 5, A and B).
Male breast cancer, in addition to being rare, is highly aggressive, with early metastases to the axillary lymph nodes(5). According to a study carried out by Gallardo et al.(2) in 303 cases of bone metastasis due to breast cancer, it was found that only 1.33% were male patients.
No specific treatment for male breast carcinoma was found in the literature. The treatment for bone metastasis from breast cancer, when there is no imminent fracture, is essentially chemotherapy and radiotherapy. Sanoo et al.(7), using combined therapy with tamoxifen, cyclophosphamide, fluorocil, morphine and medroxyprogesterone 17-acetate, concluded that this chemotherapy was effective for bone pain in 96.33% of cases. Saez et al.(6) studied the survival of patients with breast cancer metastasis who underwent resection surgery, bone graft placement, chemotherapy and use of adjuvant antineoplastic agents. The study was carried out on 20 women between 24 and 56 years of age, of which nine had complete remission and 11 had partial remission. In our opinion, the use of bone grafts in metastatic tumors is highly debatable. The treatment of pathological fracture is varied. Some factors, such as age, stage of the primary disease, size of the metastasis and the patient’s general clinical impairment, influence the prognosis and help to choose the best treatment for the fracture(1). In patients with severe impairment of the general condition or large tumor extension, when surgical possibilities are very limited, treatment may be expectant(3). If the patient is ready to undergo surgery, the following can be performed: 1) reduction and osteosynthesis with a plate and bone cement aiming for a quick solution to the fracture, 2) resection of the lesion and placement of a non-conventional endoprosthesis, providing an early return to walking, and 3) amputation in extreme cases(1). We must remember the importance of carrying out a complete physical examination on all patients so that it does not go unnoticed, as in our case, a tumor in the breast that has been evolving for several years. A thorough physical examination, including in cases where there is no suspicion of a pathological fracture, can allow for an early diagnosis of the injury, improving the prognosis. We must also highlight the importance of including, in the differential diagnosis of bone lesions suggestive of metastasis in men, breast carcinoma as the primary tumor.
Click here to see a case of hypernephroma metastasis, treated before fracture.
1. Carnelase, PG: “Malignant tumors of bone”, in Crenshaw, AH: Campbell’s operative orthopedics, St. Louis, Mosby Year Book, 1992. Chapter 10, p. 263-190.
2. Gallardo, H., Gonzales, R. & Astagno, A.: Osseous metastasis of breast cancer. Bol Acad Nal Med Nal 66: 459-471, 1988.
3. Campanacci, M.: Tumori delle ossa e delle parti molle, Bologna, Aulo Gaggi Editore, 1981. p. 456-512.
4. Pendleburg, SC, Bilous, M. & Langlands, SA: Sarcomas following radiation therapy for breast cancer: a report of three cases and a review of the literature. Int J Radiat Oncol Biol Phys 31: 405-410, 1995.
5. Robins, SL & Cotran, RS: “Mama”, in Structural and functional pathology, Rio de Janeiro, Interamericana, 1986. Chapter 27, p. 1158-1168.
6. Saez, RA, Slease, RB, Selby, GB et al: Long-term survival after autologous bone marrow transplantation for metastatic breast carcinoma. South Med J 88: 320-326, 1995.
7. Sanoo, H., Shimozuma, K., Kurebayashi, J. et al: Systemic therapeutic pain relief and quality of life of breast cancer patients with bone metastasis. Gan To Kagaku Ryoho 22 (Suppl): 10-15, 1995.
AUTHORS: PEDRO PÉRICLES RIBEIRO BAPTISTA, JOSÉ DONATO DE PROSPERO, FLORINDO VOLPE NETO, MARCOS SANMARTIN FERNANDEZ, NABIL ABISAMBRA PINILLA
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com
In recent decades, much has been discussed about the nature of gigantocellular tumors. For Geschikter and Copeland (1949)(6) and Willis (1949)(7), the gigantocellular tumor would be a neoplasm of osteoclasts in the mesenchymal stroma, given the similarity between the gigantocyte and the normal osteoclast.
Jaffe et al (1940)(8) described its origin as being derived from stromal cells. Sherman (1965)(9) stated that the bone disappeared at the site of tumor growth and the gigantocytes resulted from the fusion of stromal mesenchymal cells, taking into account the similarity between optical microscopy of stromal nuclei and giant cells. The histochemistry and tissue culture studies carried out by Schajowicz (1961)(10) did not demonstrate significant differences between tumor gigantocytes and normal osteoclasts. On the other hand, studies using electron microscopy(11) confirmed that giant cells are syncytia made up of stromal cells. Thus, the undifferentiated mesenchymal cells from the bone marrow would give rise to the tumor stroma, whose cells, in turn, when differentiating, would form clusters with the characteristics of gigantocytes. The numerous giant cells that resemble osteoclasts, in a stroma of spindle cells, are the most important elements of this tumor. The histological aspect of GCT presents characteristics common to several tumor and pseudotumor lesions(12,13), requiring joint analysis with clinical and imaging characteristics to confirm the diagnosis(14,15).









Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com

Medial access route to the hip. The access routes for the medial approach to the hip described in the literature have proven to be insufficient for the treatment of tumors that simultaneously affect the anterior, medial and posterior regions. The authors describe a medial approach, through an inguinotomy, which facilitates the resection of tumors in this area. Disinsertion of the adductor muscles is an important step in this technique, which allows for broad exposure and better tissue manipulation. There were no postoperative complications resulting from the use of this route in the nine cases in which it was used. The advantages include: ease, speed, small intraoperative bleeding, safety regarding neurovascular structures and the wide exposure it provides.
The medial approach to the coxofemoral joint is frequently used to treat congenital hip dislocation and neuromuscular disorders. Outside this scope, its use is limited and the techniques found in the world literature are few when compared to other access routes to the hip, used for the anterior, lateral and posterior approaches.
Based on a case of synovial chondromatosis, which affected the anterior, medial and posterior regions of the hip (fig. 4, AL), the senior author began using a surgical approach via medial inguinotomy, with disinsertion of the adductor muscles, different from the medial routes. described in the literature, as they do not allow, in isolation, adequate exposure of the region.
The objective of this work is to describe a medial access route to the hip, through an inguinotomy, with disinsertion of the adductor muscles, which simultaneously provides broad access to the anterior, medial and posterior regions and facilitates the resection of tumors in this location.
METHOD
The patient is placed in a horizontal supine position. It begins with asepsis of the entire region, including the abdomen, back and perineum, in addition to the entire lower limb, which is prepared to allow free movement during the operation, in order to facilitate access to the anterior regions. and posteriorly through external and internal rotation movements (fig. 4D). The lower limb on the affected side is positioned in flexion, abduction and slight external rotation, a semi-gynecological position (fig. 1). The skin incision begins medial to palpation of the femoral artery pulse, goes towards the pubic tubercle, the point of insertion of the inguinal ligament into the pubis and the center of the incision, and extends posteriorly towards the ischial tuberosity (fig. 2 ). Next, dissection is carried out through the subcutaneous cellular tissue, cauterizing the small vessels (fig. 3, A and B). The fascia incision has the same direction as the skin incision. We continue with the detachment of the pectineus muscle from the iliopubic branch, the adductor longus, adductor brevis and gracilis pubis muscles and part of the adductor magnus muscle from the ischiopubic branch (fig. 3, C and D). The obturator nerve, which passes between the pectineus muscle and the adductor longus, is protected when this muscle is reflected (fig. 3D). The iliac psoas muscle is detached from the joint capsule and isolated up to the confluence of the circumflex vessels, allowing the greatest possible exposure (fig. 3, E and F). At this point, a Langembeck or Hom-man type retractor is positioned under the iliac psoas in order to retract and protect the femoral nerve and vessels. An incision is made in the medial portion of the joint capsule (fig. 3G) and the tumor resection or the procedure in question can be continued (fig. 3H). The capsule is closed with absorbable suture. An aspiration drain is placed and the adductor muscles are reinserted, anchoring it in the periosteum. The subcutaneous cellular tissue and skin are closed with simple sutures (Fig. 4G). It is not necessary to perform any type of postoperative immobilization.
DISCUSSION
The techniques of Ludloff(9), Zazepen & Gamidov(13) and Fer-gusson(3) have traditionally been used for the medial surgical approach to the hip. These access roads,
however, they do not always meet the needs of wide exposure for resection with adequate margin of tumors in this location (figs. 2, A and B; 3, A and C), as the adductor muscles, when separated, do not allow a satisfactory visual field, mainly in adults.
The Smith-Petersen approach(12) allows access to the antero-medial region of the hip when the joint is placed in flexion and maximum external rotation, but does not expose the post-tero-medial region. In the posterior routes(2,4,7), the posterior wall of the acetabulum can make it difficult to adequately expose the femoral head. In extreme cases, the surgeon’s only alternative is hip dislocation, a dangerous procedure in terms of preserving circulation to the femoral head. In children, there is still concern about the growth physis. These factors led us to search for a technique that would allow the region to be more easily exposed, aiming for less traumatic manipulation for the tissues. The lateral approach with greater trochanter osteotomy(6), although it allows anterior and posterior access, does not expose the medial region.
The medial approach to the hip that we are describing may seem risky at first impression. This may be due to thinking based on two aspects: first, the proximity of the femoral vessels and second, the infrequent use, by orthopedists, of medial access in general. The experience acquired with resections of tumors of the obturator ring using the technique of Radley et al.(11) and with the performance of hemipelvectomies(8) made it possible to visualize this access and allowed the extrapolation of the techniques used in these cases for the treatment of tumors of the obturator ring. medial region of the hip.
The advantages of inguinotomy are several. The approach does not require major detachments or osteotomies, factors that increase postoperative morbidity. The intraoperative concern with the large femoral vessels becomes minimized, as they, when removed, are protected and, with hip flexion, move forward, moving away from the region. Intraoperative bleeding is small. The direction of the incision runs parallel to the Langerhans lines, therefore providing a good scar. Postoperative skin tension is minimal in the patient’s resting position, in which the limbs are normally in adduction. The incision site is easily covered by clothing (including swimwear) and pubic hair. The cosmetic appearance is the best possible (figs. 5 and 6).
Nine patients (Table 1) with hip tumors were treated and operated using the method described. All patients had some degree of joint limitation, with improvement in all cases after surgery. No complications were found resulting from the use of this access route. Disinsertion of the adductor muscles did not result in any deficit in adduction strength or limitation of abduction (fig. 4, HL). There were no changes in sensitivity postoperatively. The adductor muscles are reinserted into the periosteum in a similar way to the reinsertion of the abdominal muscles into the iliac crest performed in graft removal procedures.
Disinsertion of the adductor muscles is a fundamental point to allow broad exposure, given that, as it is reflected distally, it allows the retractors to be placed in a stable manner, facilitating the action of assistants. These conditions are important with regard to oncological criteria for tumor resection, considering that excessive manipulation of the retractors has the potential to spread neoplastic cells, increasing the risk of recurrence.
The oncological criteria for the resection margin of tumor lesions often require the surgeon to sacrifice neurovascular structures. With regard to the approach we are describing, ligation of the circumflex vessels is occasionally necessary. This procedure, when performed in situations where there is already compromised endostal irrigation, such as in cases of epiphysiolysis and femoral neck fractures, increases the risk of necrosis of the femoral head. However, in the case of tumor resections, when it is possible to preserve the endosteal vessels, the risk is lower.
The purpose of this work is to present an access route to the coxofemoral joint, highlighting that it is easy, quick and safe. Its use is not restricted to the treatment of tumors in the medial region of the hip. Its use can extend to other indications, such as surgery for congenital hip dislocation, resection-biopsies, synovectomies and removal of foreign bodies (such as firearm projectiles). In our opinion, this is the best way to simultaneously expose the anterior, medial and posterior regions of the hip.
1. Capener, N.: The approach to the hip joint (editorial). J Bone Joint Surg [Br] 32: 147, 1950.
2. Crenshaw, AH: Campbell’s Operative Orthopedics, 8th ed., Vol. 1,
3. JB Mosby Year Book, 1992.
4. Ferguson Jr., AB: Primary open reduction of congenital dislocation of the hip using a median adductor approach. J Bone Joint Surg [Am] 55:671, 1973.
5. Gibson, A.: Posterior exposure of the hip joint. J Bone Joint Surg [Br] 32: 183, 1950. Hardinge, K.: The direct lateral approach to the hip joint. J Bone Joint Surg [Br] 64: 17, 1982.
6. Harris, WH: A new lateral approach to the hip. J Bone Joint Surg [Am] 49:891, 1967.
7. Iyer, KM: A new posterior approach to the hip joint. Injury 13:76, 1981.
8. King, D. & Steelquist, J.: Transiliac amputation. J Bone Joint Surg 25:351, 1943.
9. Ludloff, K.: Zur blutigen Eihrenkung der Angeborenen Huftluxation. Z Orthop Chir 22: 272, 1908.
10. Osbourne, RP: The approach to the hip joint: a critical review and a suggested new route. Br J Surg 18:49, 1930-1931.
11. Radley, TJ, Liebig, CA & Brown, JR: Resection of the body of the pubic bone, the superior and inferior pubic rami, the inferior ischial ramus, and the ischial tuberosity: a surgical approach. J Bone Joint Surg [Am] 36:855, 1954.
12. Smith-Petersen, MN: A new supra-articular subperiosteal approach to the hip joint. Am J Orthop Surg 15:592, 1917.
13. Zazepen, S. & Gamidov, E.: Tumors of the lesser trochanter and their operative management. Am Dig Foreign Orthop Lit Fourth quarter: 191, 1972.
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com

Tumors of the proximal tibia, in children, can affect the growth plate and pose a challenge to further reconstruction of the bone defects resulting from tumor resection. Reconstruction methods do not always compensate the potential for bone growth in this segment. We present a new surgical technique of bone reconstruction, based on the transposition of the ipsilateral fibula with its growth plate and the use of an internal sliding fixation device, without need for microsurgical technique.
We report two patients with osteosarcoma of the proximal tibia affecting the growth cartilage who were treated with the new technique.
In both cases, bone healing, hypertrophy and longitudinal growth of the transposed fibula were documented.
This new technique preserves the blood supply of the auto-transplanted bone segment, maintaining physeal growth potential, with no need for microsurgery. The implant allows longitudinal bone growth, which was radiographically confirmed.
Case report, Level IV.
In the skeletally immature population, the proximal tibia hosts a growth plate that accounts for nearly 30 % of the final limb length in adulthood (Digby 1916). This is the second most frequent location of primary bone tumors, with the first being the distal femur (Mercuri et al. 1991). Tumors that develop in the proximal tibia before skeletal maturity can affect the growth plate and lead to discrepancies in the final length of the lower limbs (Fig. 1).
In young patients, reconstruction of bone defects resulting from tumor resection of this segment with traditional methods may show poor results after skeletal growth (Boyer et al. 1994). Some of this current methods include the replacement of the bone segment by megaprothesis, callotasis and the use of bone autograft or allograft (Saghieg et al. 2010). None of these techniques can replace the injured growth plate. Although callotasis allows bone lengthening, it may be impractical due to the need of multiple interventions for limb equalization in young children and the prolonged use of an external fixator device, which may favour infection in immunosuppressed oncological patients.
The advance of vascularized fibula autograft by microsurgical technique has allowed its use with the functioning physis in distant locations from its anatomical site (Agiza 1981; Langenskiöld 1983; Taylor et al. 1975). This has enabled the reconstruction of bone defects while keeping its growth potential (Pho et al. 1988). This technique, however, is costly and has potential complications.
In this study we describe a new surgical technique for reconstruction of bone lesions that compromise the proximal tibia and its growth plate in children and report two cases successfully treated with this technique. The patients, or their family, gave their consent for the use of their personal and medical information for the publication of this case report.
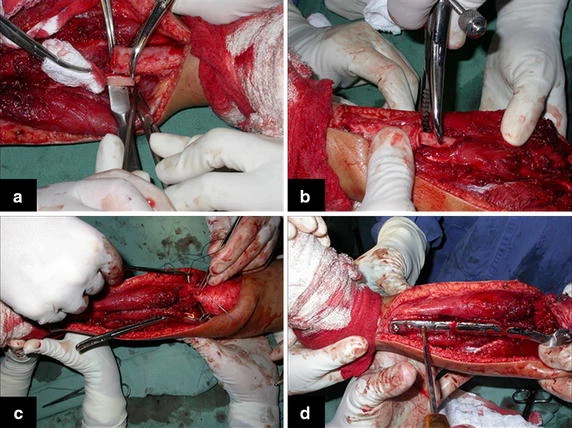
With the patient on supine position, a single incision is used. Starting above the proximal tibiofibular joint, the incision bends to the anterior tibial crest and down along it, bending again medially a few inches below the previously planned fibular osteotomy (Fig. 2a). The anterior tibialis muscle is exposed. Its perimysium is opened and the muscle is retracted laterally, leaving the inner layer of the perimysium attached to the tibial periosteum, in order to preserve the wide margin of tumor resection (Fig. 2b). The neck of the fibula is identified and the common peroneal nerve is dissected. The proximal tibiofibular joint is addressed and the joint capsule, along with the anterior and posterior ligaments, popliteal ligament, fibular collateral ligament and the femoral biceps tendon are released from the fibular head (Fig. 2c).

The proximal epiphysis of the tibia and the anterior tuberosity are isolated from the metaphyseal region (Fig. 2d). A Kirschner wire is inserted horizontally trough the epiphysis where the proximal fixation of the plate will take place. The position of the plate is checked in this moment (Fig. 3a). The tumoral bone segment to be resected is measured, and oncologic margins are added. The distal osteotomy of the tibia at the diaphyseal region is performed. The posterior muscles attached to this portion of the bone are detached proximally, leaving the epiphyseal region that will be separated from the tumor by transepiphyseal osteotomy, and preserving as much of the epiphyseal bone and articular cartilage as possible. The tumor is now completely dissected and removed (Fig. 3b, c).

The bone gap is replaced by the ipsilateral fibula, which at this moment is isolated from the tibiofibular joint and the lateral collateral ligament. Two cm of periosteum is removed from the fibular shaft where the distal osteotomy will take place (Fig. 4a). After osteotomy, this segment of the fibular bone without its periosteum will be inserted in the bone marrow of the tibial shaft (Fig. 4b). The proximal segment of the fibula is medially transferred to the center of the remaining tibial epiphysis, along with all its muscles and nurturing arteries. The cartilage of the proximal epiphysis of the fibula is gently removed, so it can allow bone consolidation between the remaining proximal tibial epiphysis and the transposed fibula (Additional file 1: Video 5). The fibular collateral ligament is reinserted to the lateral periosteum of the tibia (Fig. 4c).
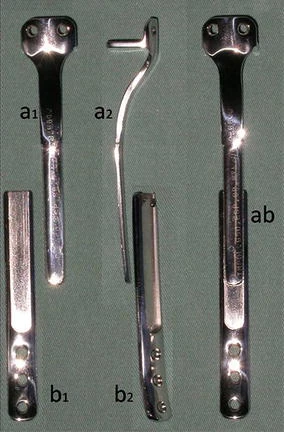
The osteosynthesis with screws is performed and a Baptista’s extendable internal fixation device, previously tailored for each case (Baptista and Yonamine 2001), is placed on the medial side of the leg (Fig. 4d). This device, made in Brazil by IMPOL, consists of two plates connected by a trapezoidal shaped rail interlocking that allows longitudinal sliding between them, but creates stability in all other directions (Additional file 2: Video 1) (Fig. 5a1, b1). The proximal plate has a platform to support the remaining portion of the tibial plateau and screw holes for attachment to the epiphysis (Fig. 5a2). The distal plate is low profile, to facilitate its coverage by the skin of the medial leg, and has holes for the screws in the tibial diaphysis (Fig. 5b2). The channels on each plate fit each other, stabilizing the junction while allowing slippage (Fig. 5ab). This device allows lengthening according to the fíbula longitudinal growth. It also provide axial compression when weight bearing starts.
The harvested fibula is interposed between the tibial epiphysis and the distal portion of the tibia. The surrounding soft tissues are reattached. After checking for vascular patency of the lateral side of the fibula, a closed vacuum wound drain is placed and the soft tissues are anatomically approximated. The limb is immobilized with an orthesis until osseous union of the proximal and distal junctions and hipertrophy of the fibula are radiographically confirmed (Additional file 3: Video 2) (Fig. 6), which usually occurs from 3 to 8 months postoperatively (Additional file 4: Video 3). Full weight bearing is authorized according to radiography consolidation and fibular hypertrophy (Additional file 5: Video 4).

A 12 year old male patient with osteosarcoma of the proximal right tibia underwent wide tumor resection, with preservation of the proximal tibial epiphysis. The proximal fibula was medially transferred with its physis to the tibial epiphysis, preserving its blood supply, and osteosynthesis was performed with an extendable internal fixation device. After surgery, the limb was kept in an orthesis.
In the fourth postoperative month, radiographic evidence of consolidation was observed and load bearing was initiated with crutches. Full weight bearing started when fibular hypertrophy was radiographically evidenced, which occured at 14 months pos operatively. During follow up the patient returned to his full activities.
In this case, we did not use fix angle screws in the proximal plate, which resulted in valgus deviation that was clinically observed and radiographically evidenced by tilting of the screws (Fig. 7a–c). The patient underwent the first scanometry of the lower limbs one year after surgery, when 0.75 cm fibular growth was observed and reorientation of the screws was done (Fig. 7b–e). Spontaneous correction of the angular deviation was clinically observed and flattening of the screws was radiographically documented, confirming the fibular longitudinal growth and the sliding of the device. The second scanometry, held 26 months postoperatively, demonstrated 1.2 cm growth of the transposed fibula (Fig. 7f). The patient is now a 26 year old man who has been followed up for 14 years without recurrences. He has equalized, satisfactory functioning lower limbs (Additional file 6: Video 6) (Fig. 8).


A 31 months old male patient presenting with Ewing’s sarcoma of the proximal right tibia underwent tumor resection with preservation of the proximal tibial epiphysis. The proximal fibula and its physis were medially transferred to the center of the tibial epiphysis, maintaining its blood supply. The osteosynthesis was performed using an extendable internal fixation device. In this case, the proximal plate was improved by creating a support to the remaining tibial plateau, aiming to improve stability and prevent angular deviations (Fig. 9b). Slots were made at every 3 mm of the distal plate to help observation of sliding between the plates, which would evidence fibular growth. After surgery, the limb was kept in an orthesis.
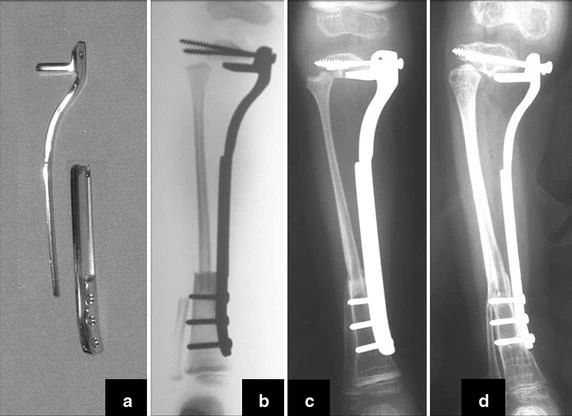
Load bearing was initiated in the third postoperative month. The patient continued on adjuvant chemotherapy and, in the fourth month, resumed walking without orthesis. During the first 8 months of follow up, approximately 0.3 cm growth of the transposed fibula was observed. Distal bone healing and initial fibular hypertrophy were radiographically confirmed (Fig. 9c, d). Non bone healing has occurred in the proximal fibula with the remnant epiphysis. Even though, full weight bearing occurred at 9 months after surgery (Additional file 5: Video 4), demonstrating the stability promoted by the Baptista’s extendable internal fixation device. After that period the patient died due to chemotherapy related complications.
Reconstruction of bone defects resulting from resection of tumors compromising the growth cartilage of the proximal tibia in children represents a challenge to the orthopedist. Due to the low frequency of these lesions, this is a rare situation, in which our technique is for a specific indication: Proximal tíbia tumors resections when the growth line must be removed for oncological reason, but the epiphysis can be preserved, in children with remnant limb growth potential.
Yoshida et al. (2010), has compared multiple reconstruction alternatives at the knee level after tumor resection. They demonstrated that when epiphyseal maintenance is feasible, the vascularized fibular graft or callotasis techniques offers the highest score in the MSTS rating system (Enneking et al. 1993).
Distraction osteogenesis with external fixator eliminates the need of graft and allows padding of the bone defects created by tumor resection through callostasis. It requires, however, long periods with an external fixator device, which increases the risk of infection in patients potentially immunosuppressed by adjuvant oncological treatment (Kapukaya et al. 2000).
Bone grafts have been used for reconstruction of proximal tibial resections, especially in cases where the tibial epiphysis can be preserved (Honoki et al. 2008), which occurs in up to 20 % of cases (Norton et al. 1991; Simon and Bos 1980). When the graft is not vascularized, the technique presents high rates of fracture or non-union, and it does not prevent further limb discrepancy (Muscolo et al. 2004). Weitao et al. (2012) reported the use of allograft in the proximal tibia in 5 patients after tumor resection preserving the epiphysis. Delayed bone healing in Allograft-host junction were seen in all cases.
Transposition of the fibula shows advantages over the allograft in the bone healing process. Since it is a bone-muscle flap with natural vascularization, bone turnover is preserved and actively participates in the process of bone healing, while the growth potential of the physis is maintained. As seen in Figs. 7 and 9, the fibula undergoes progressive hypertrophy and strengthening, in contrast to allograft, which may fail even years after integration (Date et al. 1996; Hriscu et al. 2006).
The transfer of the fibula with its growth plate as a reconstruction method requires long term rehabilitation and late resuming of loadbearing ambulation, until bone healing of the tibia and the transposed fibula occurs. Hypertrophy of the fibula, which was reported in our two cases, evidences that the bone has achieved enough resistance required for loadbearing. Since this is a biological reconstruction method, once consolidation and hypertrophy occur, it can be considered a definitive solution, carried out with a single surgical procedure. The preservation of the proximal epiphysis of the tibia while maintaining the articular surface of the knee by trans epiphyseal osteotomy represents a mechanical advantage. It is also a necessary condition to use a fibular transposition. The maintenance of longitudinal growth of the transposed fibular segment, as documented in our two patients, is of major importance, since it can prevent or minimize the final discrepancy of the lower limbs length after growth.
Capanna et al. (2007) presented a original solution for long bones intercalary defects reconstruction associating massive allograft with vascularized fibular autograft. Good results were presented in 57 patients with proximal tibia reconstruction, nevertheless this technique does not address final limb discrepancy. The authors developed a good alternative to reconstructions of bone defect of the proximal tibia, but require microsurgery technique, which increases the cost of the procedure and the availability of bone allograft compatible in size with the patient, which is not widely available in some countries.
Our technique has the advantage to waive any method of vascular reconstruction of the fibular segment, since vessels are preserved. Fibular hypertrophy and longitudinal growth of the transplanted bone segments were observed in the two reported cases. Distal bone healing was succeeded in both cases. Proximally, there was a non union in the second case, due to the non resection of the proximal fibular articular cartilage which is essential for bone healing. This patient was schedule to a second procedure to resect the articular cartilage of the proximal fibula, but he had a clinical complication, from chemotherapy, which led to death. During the first 8 months after surgery, however, growth of at least 0.3 cm of the transposed fibula was documented, suggesting preservation of the growth potential (Fig. 9).
The first patient developed a valgus deformity of the right knee in the immediate postoperative period, which was corrected within the first post-operative year, after bone growth and correction of slope of the screws (Fig. 7). Long term resolution of the tibial reconstruction defect was observed in this patient, as documented by the equal length and normal function of lower limbs in adulthood. In spite of the restricted indication, we believe that our technique can positively affect the long term outcome of young patients undergoing reconstruction of proximal tibial defects.
Reconstruction of the proximal tibia with a megaprosthesis represents a therapeutic option when epiphysis must be resected. It allows limb preservation and early ambulation but High rates of complications have been reported such as infection, aseptic loosening, mechanical failure, and limitation to physical activities (Saghieg et al. 2010; Gosheger et al. 2006; Campanacci et al. 2010; Fang et al. 2013). This method requires multiple surgical procedures for revisions, reaching 42 % implant failures in 10 years follow up (Jeys et al. 2008). When epiphyseal maintenance is feasible, megaprosthesis has fewer indications. When early ambulation is priority for low expectation of life patients.
The authors believe the excellent longterm results in the first case and the ability to restore limb growth potential in both cases, avoiding further salvage surgical procedures, justify the application of this meticulous technique. The extensible internal fixation device stabilizes the reconstruction with the ipsilateral fibula and allows bone growth through sliding of the plates.
The purpose technique is indicated in intercalary proximal tibial resection, when the growth plate is removed for oncological purpose, in young children. Especially with high growth potential. The technique is not indicated in cases of low expectation of life due to the time required to initiate ambulation. In these situations a megaprosthesis might be preferred. More patients should be included on future studies to validate the reproducibility of this new technique.
Autor : Prof. Dr. Pedro Péricles Ribeiro Baptista
Oncocirurgia Ortopédica do Instituto do Câncer Dr. Arnaldo Vieira de Carvalho
Consultório: Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – S.P.
Fone:+55 11 3231-4638 Cel:+55 11 99863-5577 Email: drpprb@gmail.com
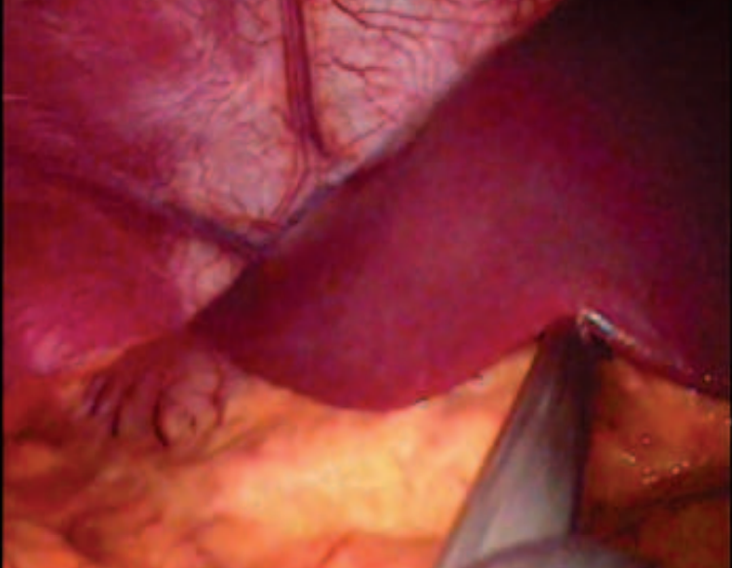
Technical Aspects of Laparoscopic . Situs inversus is a rare anomaly characterized by transposition of organs to the opposite side of the body. We report a 16-
year-old woman with known situs inversus totalis and gallstone disease who underwent a successful laparoscopic
cholecystectomy. Diagnostic and technical challenges of the operation are discussed.
INTRODUCTION
Situs inversus is a autosomal recessive morphogenetic abnormality, characterized by the transposition of the abdominal viscera to the opposite side.1 This inversion of the topography can occur in the abdominal cavity and the chest or, more rarely, in one of the two. Its incidence is estimated at 1:5,000 to 1:20,000 live births.2 The clinical diagnosis of gallstones in these patients is more difficult because the clinical presentation is confusing, especially because of the pain localized to the left hypochondrium. There is no evidence showing a higher incidence of gallstones in people with situs inversus than in those with the orthotopic topography of the abdominal viscera.2 Several studies have shown that laparoscopic cholecystectomy is safe in these patients, however, due to the rarity of this condition, there is no standardization of procedure’s technique.1-5 Our objective is to present the case of a women with situs inversus and cholelithiasis who underwent laparoscopic cholecystectomy and discuss the technique used.
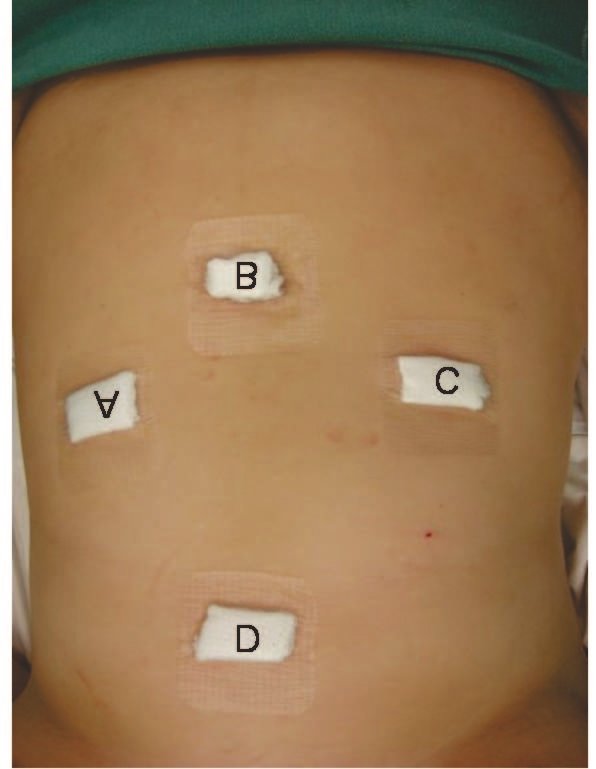
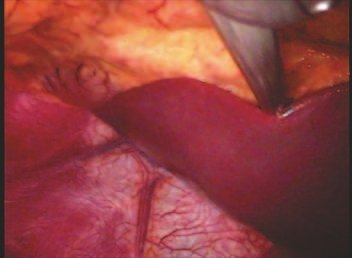


Autor : Prof. Dr. Pedro Péricles Ribeiro Baptista
Oncocirurgia Ortopédica do Instituto do Câncer Dr. Arnaldo Vieira de Carvalho
Consultório: Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – S.P.
Fone:+55 11 3231-4638 Cel:+55 11 99863-5577 Email: drpprb@gmail.com
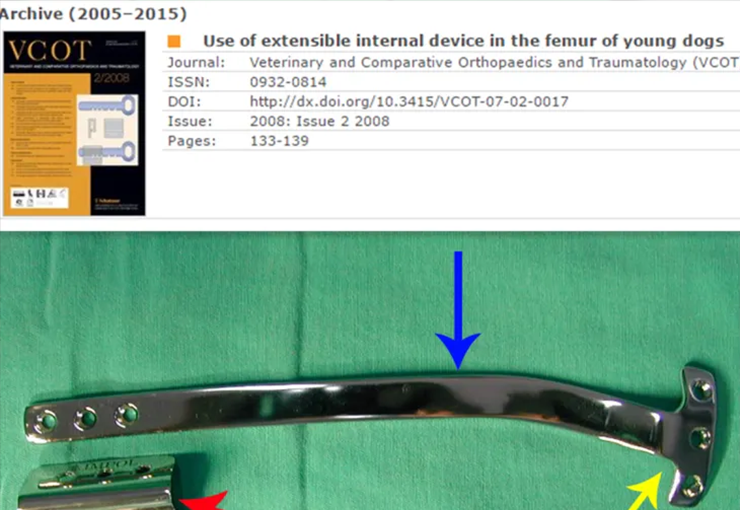
Use of extensible internal device in the femur of young dogs. 1,2Departments of Veterinary Surgery and Anesthesiology, and 5Animal Reproduction and Radiology, School of Veterinary Medicine and Animal Science, São Paulo State University (UNESP), Botucatu Campus, São Paulo, Brazil 3,4Department of Orthopedics and Traumatology, Santa Casa Medical School, São Paulo, Brazil 6Department of Basic Sciences, School of Animal Science, Pirassununga Campus, São Paulo University (USP), São Paulo, Brazil
An extensible internal device (EID) was developed to preserve growth plate during the treatment of fracture complications or segmental bone loss from tumour resection in children. Since this type of extensible, transphyseal, internal fixation device has only been used in a few paediatric cases; the aim of this study was to evaluate an in vivo canine study, a surgical application of this device, and its interference with longitudinal growth of the non-fractured distal femur. Ten clinically healthy two- to three-month-old poodles weighing 1.5–2.3 kg were used. Following a medial approach to the right distal femur, one extremity of the EID, similar to a T-plate, was fixed in the femoral condyle with two cortical screws placed below the growth plate. The other extremity, consisting of an adaptable brim with two screw holes and a plate guide, was fixed in the third distal of the femoral diaphysis with two cortical screws. The EID was removed 180 days after application. All of the dogs demonstrated full weight-bearing after surgery. The values of thigh and stifle circumferences, and stifle joint motion range did not show any difference between operated and control hindlimbs. The plate slid in the device according to longitudinal bone growth, in all but one dog. In this dog, a 10.5% shortening of the femoral shaft was observed due to a lack of EID sliding. The other dogs had the same longitudinal lengths in both femurs. The EID permits longitudinal bone growth without blocking the distal femur
Autor : Prof. Dr. Pedro Péricles Ribeiro Baptista
Oncocirurgia Ortopédica do Instituto do Câncer Dr. Arnaldo Vieira de Carvalho
Consultório: Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – S.P.
Fone:+55 11 3231-4638 Cel:+55 11 99863-5577 Email: drpprb@gmail.com
Este livro sobre Oncologia e Oncocirurgia Ortopédica disponível neste site: www.oncocirurgia.com.br Inclui aulas acadêmicas, palestras proferidas em congressos nacionais e internacionais, trabalhos publicados, discussões de casos, procedimentos cirúrgicos realizados e técnicas próprias desenvolvidas.
O formato digital foi escolhido porque a web permite a inclusão de textos com inúmeros recursos visuais, como imagens e vídeos, que não seriam possíveis em um livro impresso.
O conteúdo é destinado a estudantes, profissionais da saúde e ao público em geral interessado na área.
Fale agora via WhatsApp