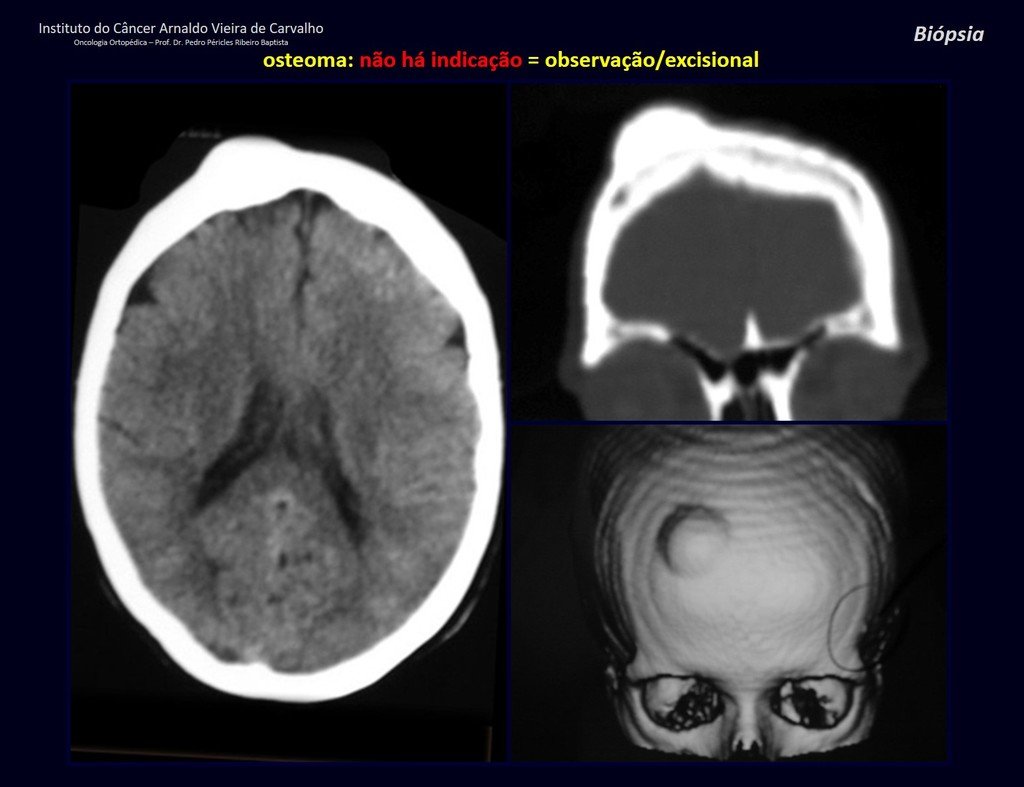
Patients B : Figure 5.
At the outpatient clinic, the resident asks:
– “By which access route should we perform the biopsy?”
I see the image and ask: – How old is the patient?
– “Um… Dona Maria, how old are you?”
I reflect in silence, evaluating the learner’s lack of knowledge. The patient responds 67 years old DOCTOR!
… Sixty-seven years, multiple lesions, metastasis? Multiple myeloma? Brown tumor of hyperparathyroidism? – How long has she had symptoms?
– “Um… Dona Maria, how long have you had this problem?”
In the medical record I see symptoms of pain in the ischial tuberosity noted , measurements of Ca ++ , P ++ , FA, Na + , K + , protein electrophoresis, blood count, ESR, blood glucose, urea, creatinine, ultrasound, x-rays,…, …
When examining the patient, I observed that the “tumor” is anterior , in the inguinal region, and not posterior , as noted in the medical record, “ischial tuberosity”. The patient had not been examined !!! She had an inguinal-crural hernia. Pelvic x-ray images represent gas from the intestine. The “biopsy” would result in intestinal perforation. The physical examination made the diagnosis.
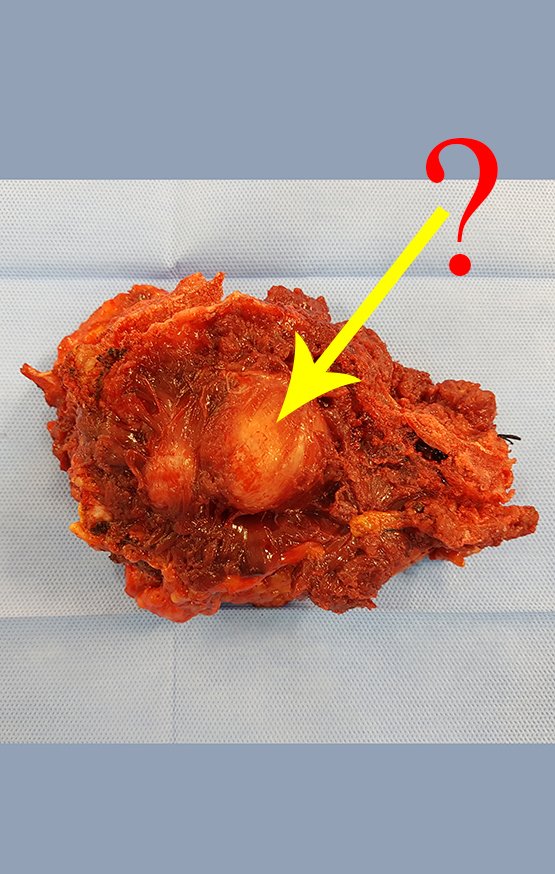
Patient C : Figure 6.
Passing through the emergency room, the person on duty asks:
– “Doctor, what tumor do you think this patient has? Can we schedule the biopsy?”
The resident knew nothing about the history and had only taken the frontal x-ray!!! When asked, the patient reports that the inflammatory symptoms began six months ago, with hot pain and the release of purulent secretions. When it was open, secreting, the symptoms improved. When he closed the fistula it started to swell, hurt and he had a fever.
With difficulty, as the patient often withholds information, we learned that he had been injured in the thigh two years ago, when he jumped over the guardrail of a house, which bled a lot, but did not seek treatment ( clinical history ) . We requested a lateral x-ray which confirmed that it was a foreign body. The spear tip of the grid was surrounded by solid periosteal reaction, giving the false impression of a sclerotic tumor. Appropriate imaging confirmed the diagnosis.