Metastasis in the femur from male breast carcinoma
INTRODUCTION
Breast cancer is a neoplasm that most frequently originates from the excretory ducts of the gland and also from its acini. It occupies a prominent place as a cause
of death in women, but in men it is very rare. For every 100 cases of breast cancer, only one is male. It affects the adult age group, generally over 50 years old. Due to the scarcity of breast parenchyma in men, cancer infiltrates more quickly and adheres to the skin with ulceration(3,5). It behaves exactly as in invasive ductal carcinomas in women, but generally presents with minor desmoplasia. The spread is the same as in women, with
early metastases in the axillary nodes. Metastases in the lungs, brain, bones and liver are also frequent, via the hematogenous route. The femur is the most affected bone(3). The objective of this work is to report a rare case of bone metastasis from male breast carcinoma, due to its rarity and propensity for misdiagnosis.
CASE REPORT
A 69-year-old male patient was admitted to the emergency room of the Department of Orthopedics and Traumatology of Santa Casa de São Paulo, with a history of
falling to the ground four hours ago, with pain and functional impotence of the right lower limb. At admission, shortening and deformity in external rotation of the right lower limb were observed
. At the time, no other abnormalities were noted on physical examination.
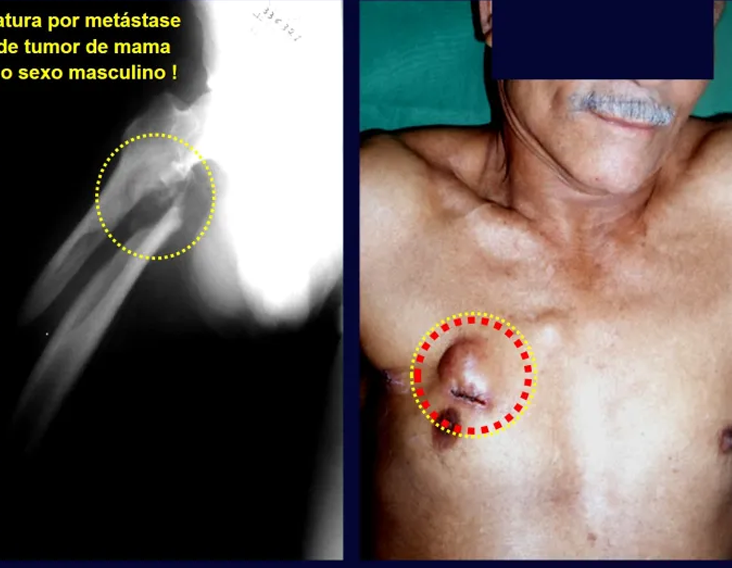
On radiographic examination, in the anteroposterior projection of the pelvis and lateral aspect of the right hip (Fig. 1), a long oblique fracture without comminution or other bone injury was observed in the subtrochanteric region of the right femur. Biochemical and hematological blood analyses, chest x-rays and electrocardiogram were normal. The patient underwent anatomical reduction and osteosynthesis of the fracture with a 95º angled plate (fig. 2).


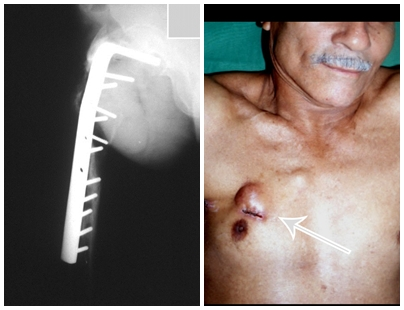
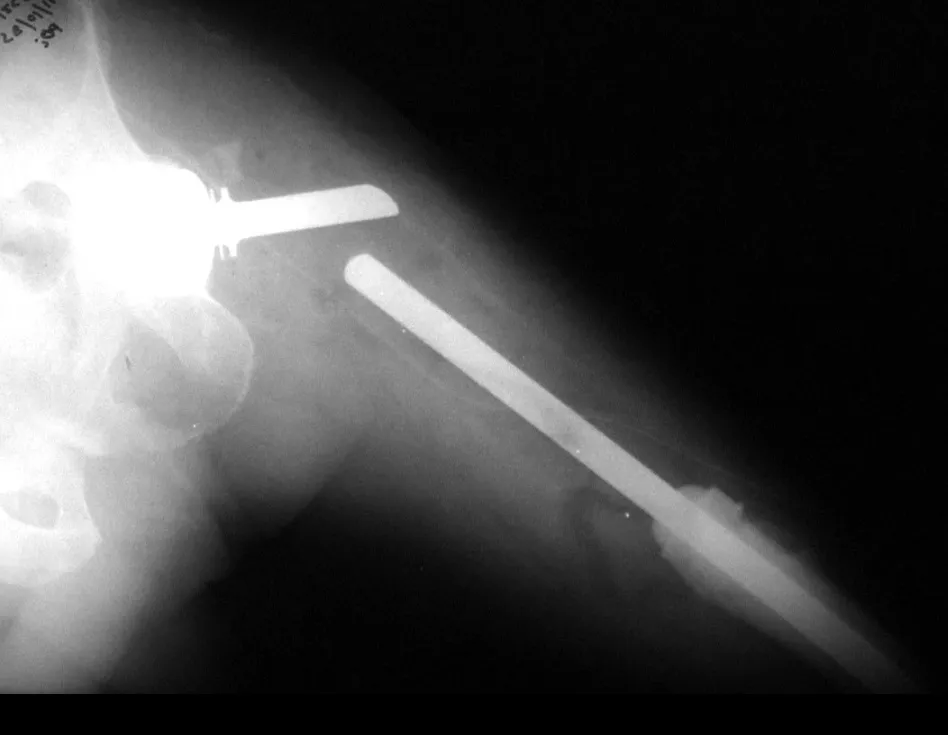
The patient underwent a trocar biopsy of the lesion in the femur and an incisional biopsy of the mass in the breast. The results of the anatomopathological examinations were as follows: metastasis of adenocarcinoma in the femur and infiltrative ductal carcinoma of the breast. A resection of the proximal third of the right femur was performed and a non-conventional Fabroni endoprosthesis (ENCF) was placed (fig. 6). The evolution in the immediate postoperative period was satisfactory. Two weeks after surgery, the patient began chemotherapy with cyclophosphamide, fluoracil and farmorubicin with the aim of facilitating breast resection and lymph node emptying. Currently (six months post-operatively), the patient, still undergoing chemotherapy, has a limp with the aid of crutches, a normal neurological examination and the following mobility of the right hip: 90º of flexion,
–15º of extension, 30º of abduction , 20º of adduction, 60º of external rotation and 0º of internal rotation (fig. 5, A and B).
DISCUSSION
Male breast cancer, in addition to being rare, is highly aggressive, with early metastases to the axillary lymph nodes(5). According to a study carried out by Gallardo et al.(2) in 303 cases of bone metastasis due to breast cancer, it was found that only 1.33% were male patients.
No specific treatment for male breast carcinoma was found in the literature. The treatment for bone metastasis from breast cancer, when there is no imminent fracture, is essentially chemotherapy and radiotherapy. Sanoo et al.(7), using combined therapy with tamoxifen, cyclophosphamide, fluorocil, morphine and medroxyprogesterone 17-acetate, concluded that this chemotherapy was effective for bone pain in 96.33% of cases. Saez et al.(6) studied the survival of patients with breast cancer metastasis who underwent resection surgery, bone graft placement, chemotherapy and use of adjuvant antineoplastic agents. The study was carried out on 20 women between 24 and 56 years of age, of which nine had complete remission and 11 had partial remission. In our opinion, the use of bone grafts in metastatic tumors is highly debatable. The treatment of pathological fracture is varied. Some factors, such as age, stage of the primary disease, size of the metastasis and the patient’s general clinical impairment, influence the prognosis and help to choose the best treatment for the fracture(1). In patients with severe impairment of the general condition or large tumor extension, when surgical possibilities are very limited, treatment may be expectant(3). If the patient is ready to undergo surgery, the following can be performed: 1) reduction and osteosynthesis with a plate and bone cement aiming for a quick solution to the fracture, 2) resection of the lesion and placement of a non-conventional endoprosthesis, providing an early return to walking, and 3) amputation in extreme cases(1). We must remember the importance of carrying out a complete physical examination on all patients so that it does not go unnoticed, as in our case, a tumor in the breast that has been evolving for several years. A thorough physical examination, including in cases where there is no suspicion of a pathological fracture, can allow for an early diagnosis of the injury, improving the prognosis. We must also highlight the importance of including, in the differential diagnosis of bone lesions suggestive of metastasis in men, breast carcinoma as the primary tumor.
Click here to see a case of hypernephroma metastasis, treated before fracture.
REFERENCES
1. Carnelase, PG: “Malignant tumors of bone”, in Crenshaw, AH: Campbell’s operative orthopedics, St. Louis, Mosby Year Book, 1992. Chapter 10, p. 263-190.
2. Gallardo, H., Gonzales, R. & Astagno, A.: Osseous metastasis of breast cancer. Bol Acad Nal Med Nal 66: 459-471, 1988.
3. Campanacci, M.: Tumori delle ossa e delle parti molle, Bologna, Aulo Gaggi Editore, 1981. p. 456-512.
4. Pendleburg, SC, Bilous, M. & Langlands, SA: Sarcomas following radiation therapy for breast cancer: a report of three cases and a review of the literature. Int J Radiat Oncol Biol Phys 31: 405-410, 1995.
5. Robins, SL & Cotran, RS: “Mama”, in Structural and functional pathology, Rio de Janeiro, Interamericana, 1986. Chapter 27, p. 1158-1168.
6. Saez, RA, Slease, RB, Selby, GB et al: Long-term survival after autologous bone marrow transplantation for metastatic breast carcinoma. South Med J 88: 320-326, 1995.
7. Sanoo, H., Shimozuma, K., Kurebayashi, J. et al: Systemic therapeutic pain relief and quality of life of breast cancer patients with bone metastasis. Gan To Kagaku Ryoho 22 (Suppl): 10-15, 1995.
AUTHORS: PEDRO PÉRICLES RIBEIRO BAPTISTA, JOSÉ DONATO DE PROSPERO, FLORINDO VOLPE NETO, MARCOS SANMARTIN FERNANDEZ, NABIL ABISAMBRA PINILLA
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com