
Medial access route to the hip for resection of tumor lesions
Medial access route to the hip. The access routes for the medial approach to the hip described in the literature have proven to be insufficient for the treatment of tumors that simultaneously affect the anterior, medial and posterior regions. The authors describe a medial approach, through an inguinotomy, which facilitates the resection of tumors in this area. Disinsertion of the adductor muscles is an important step in this technique, which allows for broad exposure and better tissue manipulation. There were no postoperative complications resulting from the use of this route in the nine cases in which it was used. The advantages include: ease, speed, small intraoperative bleeding, safety regarding neurovascular structures and the wide exposure it provides.
The medial approach to the coxofemoral joint is frequently used to treat congenital hip dislocation and neuromuscular disorders. Outside this scope, its use is limited and the techniques found in the world literature are few when compared to other access routes to the hip, used for the anterior, lateral and posterior approaches.
Based on a case of synovial chondromatosis, which affected the anterior, medial and posterior regions of the hip (fig. 4, AL), the senior author began using a surgical approach via medial inguinotomy, with disinsertion of the adductor muscles, different from the medial routes. described in the literature, as they do not allow, in isolation, adequate exposure of the region.
The objective of this work is to describe a medial access route to the hip, through an inguinotomy, with disinsertion of the adductor muscles, which simultaneously provides broad access to the anterior, medial and posterior regions and facilitates the resection of tumors in this location.
METHOD
The patient is placed in a horizontal supine position. It begins with asepsis of the entire region, including the abdomen, back and perineum, in addition to the entire lower limb, which is prepared to allow free movement during the operation, in order to facilitate access to the anterior regions. and posteriorly through external and internal rotation movements (fig. 4D). The lower limb on the affected side is positioned in flexion, abduction and slight external rotation, a semi-gynecological position (fig. 1). The skin incision begins medial to palpation of the femoral artery pulse, goes towards the pubic tubercle, the point of insertion of the inguinal ligament into the pubis and the center of the incision, and extends posteriorly towards the ischial tuberosity (fig. 2 ). Next, dissection is carried out through the subcutaneous cellular tissue, cauterizing the small vessels (fig. 3, A and B). The fascia incision has the same direction as the skin incision. We continue with the detachment of the pectineus muscle from the iliopubic branch, the adductor longus, adductor brevis and gracilis pubis muscles and part of the adductor magnus muscle from the ischiopubic branch (fig. 3, C and D). The obturator nerve, which passes between the pectineus muscle and the adductor longus, is protected when this muscle is reflected (fig. 3D). The iliac psoas muscle is detached from the joint capsule and isolated up to the confluence of the circumflex vessels, allowing the greatest possible exposure (fig. 3, E and F). At this point, a Langembeck or Hom-man type retractor is positioned under the iliac psoas in order to retract and protect the femoral nerve and vessels. An incision is made in the medial portion of the joint capsule (fig. 3G) and the tumor resection or the procedure in question can be continued (fig. 3H). The capsule is closed with absorbable suture. An aspiration drain is placed and the adductor muscles are reinserted, anchoring it in the periosteum. The subcutaneous cellular tissue and skin are closed with simple sutures (Fig. 4G). It is not necessary to perform any type of postoperative immobilization.
DISCUSSION
The techniques of Ludloff(9), Zazepen & Gamidov(13) and Fer-gusson(3) have traditionally been used for the medial surgical approach to the hip. These access roads,
however, they do not always meet the needs of wide exposure for resection with adequate margin of tumors in this location (figs. 2, A and B; 3, A and C), as the adductor muscles, when separated, do not allow a satisfactory visual field, mainly in adults.
The Smith-Petersen approach(12) allows access to the antero-medial region of the hip when the joint is placed in flexion and maximum external rotation, but does not expose the post-tero-medial region. In the posterior routes(2,4,7), the posterior wall of the acetabulum can make it difficult to adequately expose the femoral head. In extreme cases, the surgeon’s only alternative is hip dislocation, a dangerous procedure in terms of preserving circulation to the femoral head. In children, there is still concern about the growth physis. These factors led us to search for a technique that would allow the region to be more easily exposed, aiming for less traumatic manipulation for the tissues. The lateral approach with greater trochanter osteotomy(6), although it allows anterior and posterior access, does not expose the medial region.
The medial approach to the hip that we are describing may seem risky at first impression. This may be due to thinking based on two aspects: first, the proximity of the femoral vessels and second, the infrequent use, by orthopedists, of medial access in general. The experience acquired with resections of tumors of the obturator ring using the technique of Radley et al.(11) and with the performance of hemipelvectomies(8) made it possible to visualize this access and allowed the extrapolation of the techniques used in these cases for the treatment of tumors of the obturator ring. medial region of the hip.
The advantages of inguinotomy are several. The approach does not require major detachments or osteotomies, factors that increase postoperative morbidity. The intraoperative concern with the large femoral vessels becomes minimized, as they, when removed, are protected and, with hip flexion, move forward, moving away from the region. Intraoperative bleeding is small. The direction of the incision runs parallel to the Langerhans lines, therefore providing a good scar. Postoperative skin tension is minimal in the patient’s resting position, in which the limbs are normally in adduction. The incision site is easily covered by clothing (including swimwear) and pubic hair. The cosmetic appearance is the best possible (figs. 5 and 6).
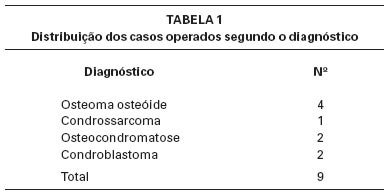
Nine patients (Table 1) with hip tumors were treated and operated using the method described. All patients had some degree of joint limitation, with improvement in all cases after surgery. No complications were found resulting from the use of this access route. Disinsertion of the adductor muscles did not result in any deficit in adduction strength or limitation of abduction (fig. 4, HL). There were no changes in sensitivity postoperatively. The adductor muscles are reinserted into the periosteum in a similar way to the reinsertion of the abdominal muscles into the iliac crest performed in graft removal procedures.
Disinsertion of the adductor muscles is a fundamental point to allow broad exposure, given that, as it is reflected distally, it allows the retractors to be placed in a stable manner, facilitating the action of assistants. These conditions are important with regard to oncological criteria for tumor resection, considering that excessive manipulation of the retractors has the potential to spread neoplastic cells, increasing the risk of recurrence.
The oncological criteria for the resection margin of tumor lesions often require the surgeon to sacrifice neurovascular structures. With regard to the approach we are describing, ligation of the circumflex vessels is occasionally necessary. This procedure, when performed in situations where there is already compromised endostal irrigation, such as in cases of epiphysiolysis and femoral neck fractures, increases the risk of necrosis of the femoral head. However, in the case of tumor resections, when it is possible to preserve the endosteal vessels, the risk is lower.
The purpose of this work is to present an access route to the coxofemoral joint, highlighting that it is easy, quick and safe. Its use is not restricted to the treatment of tumors in the medial region of the hip. Its use can extend to other indications, such as surgery for congenital hip dislocation, resection-biopsies, synovectomies and removal of foreign bodies (such as firearm projectiles). In our opinion, this is the best way to simultaneously expose the anterior, medial and posterior regions of the hip.
1. Capener, N.: The approach to the hip joint (editorial). J Bone Joint Surg [Br] 32: 147, 1950.
2. Crenshaw, AH: Campbell’s Operative Orthopedics, 8th ed., Vol. 1,
3. JB Mosby Year Book, 1992.
4. Ferguson Jr., AB: Primary open reduction of congenital dislocation of the hip using a median adductor approach. J Bone Joint Surg [Am] 55:671, 1973.
5. Gibson, A.: Posterior exposure of the hip joint. J Bone Joint Surg [Br] 32: 183, 1950. Hardinge, K.: The direct lateral approach to the hip joint. J Bone Joint Surg [Br] 64: 17, 1982.
6. Harris, WH: A new lateral approach to the hip. J Bone Joint Surg [Am] 49:891, 1967.
7. Iyer, KM: A new posterior approach to the hip joint. Injury 13:76, 1981.
8. King, D. & Steelquist, J.: Transiliac amputation. J Bone Joint Surg 25:351, 1943.
9. Ludloff, K.: Zur blutigen Eihrenkung der Angeborenen Huftluxation. Z Orthop Chir 22: 272, 1908.
10. Osbourne, RP: The approach to the hip joint: a critical review and a suggested new route. Br J Surg 18:49, 1930-1931.
11. Radley, TJ, Liebig, CA & Brown, JR: Resection of the body of the pubic bone, the superior and inferior pubic rami, the inferior ischial ramus, and the ischial tuberosity: a surgical approach. J Bone Joint Surg [Am] 36:855, 1954.
12. Smith-Petersen, MN: A new supra-articular subperiosteal approach to the hip joint. Am J Orthop Surg 15:592, 1917.
13. Zazepen, S. & Gamidov, E.: Tumors of the lesser trochanter and their operative management. Am Dig Foreign Orthop Lit Fourth quarter: 191, 1972.
Author: Prof. Dr. Pedro Péricles Ribeiro Baptista
Orthopedic Oncosurgery at the Dr. Arnaldo Vieira de Carvalho Cancer Institute
Office : Rua General Jardim, 846 – Cj 41 – Cep: 01223-010 Higienópolis São Paulo – SP
Phone: +55 11 3231-4638 Cell:+55 11 99863-5577 Email: drpprb@gmail.com